Agung Ary Wibowo, Oscar Tri Joko Putra, Zairin Noor Helmi, Hery Poerwosusanta, Tjahyo Kelono Utomo, Kenanga Marwan Sikumbang
{"title":"预测腹腔镜胆囊切除术困难的评分系统:一项为期五年的横断面研究。","authors":"Agung Ary Wibowo, Oscar Tri Joko Putra, Zairin Noor Helmi, Hery Poerwosusanta, Tjahyo Kelono Utomo, Kenanga Marwan Sikumbang","doi":"10.1155/2022/3530568","DOIUrl":null,"url":null,"abstract":"Background Laparoscopic cholecystectomy since long time already has become the preferred method because laparoscopic cholecystectomy has many advantages compared to standard open cholecystectomy. However, since it has associated with a higher risk of complication, preoperative prediction of risk factors is needed to assess the intraoperative difficulties. Various scoring systems have a role in predicting intraoperative difficulties; however, there is a need to find a consistent and reliable predictive system. Aim To validate a preoperative scoring system that will predict difficult laparoscopic cholecystectomy. Design of the Study. Nonrandomized retrospective descriptive study. Setting. Department of General Surgery, Lambung Mangkurat Univeristy Ulin Referral Hospital, Banjarmasin, Kalimantan Selatan, Indonesia. Methodology. A preoperative score was given to all the patients (134 patients from January 2015–December 2020) based on history, clinical examination, and sonographic findings. Using ROC curve, the cutoff for easy—difficult was 3.5 and difficult—very difficult was 7.5. The scores were compared in each patient to conclude the practicality of the preoperative predictive score. SPSS version 25 was used to analyze the data. Results History of hospitalization for acute cholecystitis (p ≤ 0.001), high BMI (p=0.002), abdominal scar (p=0.005), palpable gallbladder (p ≤ 0.001), thick gallbladder wall (p ≤ 0.001), and leucocyte (p ≤ 0.001) were considered as the significant factors that predict difficult laparoscopic cholecystectomy. Sensitivity and specificity for easy—difficult cutoff of the scoring method were 72.6% and 87.5%, respectively, with the area under the ROC curve being 0.849. Sensitivity and specificity for difficult—very difficult cutoff of the scoring method were 70.0% and 84.5%, respectively, with the area under the ROC curve being 0.779. Conclusion The preoperative scoring system evaluated in the study is reliable and beneficial in predicting the difficulty of laparoscopic cholecystectomy. However, further randomized prospective multicentric studies with large sample sizes are required to validate the efficiency of the scoring system.","PeriodicalId":45110,"journal":{"name":"Minimally Invasive Surgery","volume":" ","pages":"3530568"},"PeriodicalIF":1.3000,"publicationDate":"2022-09-06","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9470297/pdf/","citationCount":"1","resultStr":"{\"title\":\"A Scoring System to Predict Difficult Laparoscopic Cholecystectomy: A Five-Year Cross-Sectional Study.\",\"authors\":\"Agung Ary Wibowo, Oscar Tri Joko Putra, Zairin Noor Helmi, Hery Poerwosusanta, Tjahyo Kelono Utomo, Kenanga Marwan Sikumbang\",\"doi\":\"10.1155/2022/3530568\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"Background Laparoscopic cholecystectomy since long time already has become the preferred method because laparoscopic cholecystectomy has many advantages compared to standard open cholecystectomy. However, since it has associated with a higher risk of complication, preoperative prediction of risk factors is needed to assess the intraoperative difficulties. Various scoring systems have a role in predicting intraoperative difficulties; however, there is a need to find a consistent and reliable predictive system. Aim To validate a preoperative scoring system that will predict difficult laparoscopic cholecystectomy. Design of the Study. Nonrandomized retrospective descriptive study. Setting. Department of General Surgery, Lambung Mangkurat Univeristy Ulin Referral Hospital, Banjarmasin, Kalimantan Selatan, Indonesia. Methodology. A preoperative score was given to all the patients (134 patients from January 2015–December 2020) based on history, clinical examination, and sonographic findings. Using ROC curve, the cutoff for easy—difficult was 3.5 and difficult—very difficult was 7.5. The scores were compared in each patient to conclude the practicality of the preoperative predictive score. SPSS version 25 was used to analyze the data. Results History of hospitalization for acute cholecystitis (p ≤ 0.001), high BMI (p=0.002), abdominal scar (p=0.005), palpable gallbladder (p ≤ 0.001), thick gallbladder wall (p ≤ 0.001), and leucocyte (p ≤ 0.001) were considered as the significant factors that predict difficult laparoscopic cholecystectomy. Sensitivity and specificity for easy—difficult cutoff of the scoring method were 72.6% and 87.5%, respectively, with the area under the ROC curve being 0.849. Sensitivity and specificity for difficult—very difficult cutoff of the scoring method were 70.0% and 84.5%, respectively, with the area under the ROC curve being 0.779. Conclusion The preoperative scoring system evaluated in the study is reliable and beneficial in predicting the difficulty of laparoscopic cholecystectomy. However, further randomized prospective multicentric studies with large sample sizes are required to validate the efficiency of the scoring system.\",\"PeriodicalId\":45110,\"journal\":{\"name\":\"Minimally Invasive Surgery\",\"volume\":\" \",\"pages\":\"3530568\"},\"PeriodicalIF\":1.3000,\"publicationDate\":\"2022-09-06\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9470297/pdf/\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Minimally Invasive Surgery\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1155/2022/3530568\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2022/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"SURGERY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Minimally Invasive Surgery","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2022/3530568","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 1
摘要
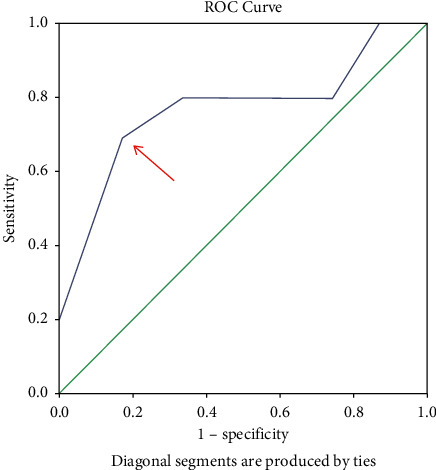
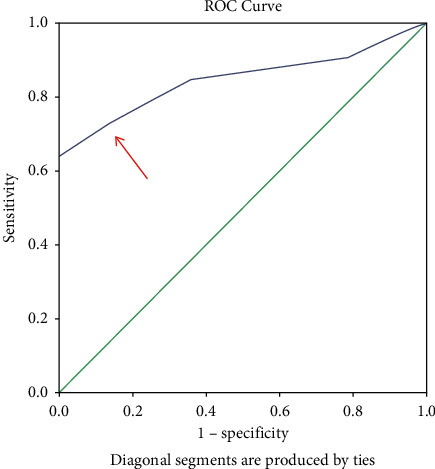
背景:由于腹腔镜胆囊切除术与标准开腹胆囊切除术相比具有许多优点,长期以来腹腔镜胆囊切除术已成为首选方法。然而,由于它与较高的并发症风险相关,术前需要预测危险因素以评估术中困难。各种评分系统在预测术中困难方面具有重要作用;然而,有必要找到一个一致和可靠的预测系统。目的:验证一种预测腹腔镜胆囊切除术难度的术前评分系统。研究的设计。非随机回顾性描述性研究。设置。兰邦曼库拉特大学乌林转诊医院普外科,班加马辛,加里曼丹塞拉丹,印度尼西亚。方法。所有患者(134例,2015年1月- 2020年12月)根据病史、临床检查和超声检查结果进行术前评分。采用ROC曲线,易-难组的截止值为3.5,难-极难组的截止值为7.5。比较每位患者的评分,得出术前预测评分的实用性。采用SPSS version 25对数据进行分析。结果:急性胆囊炎住院史(p≤0.001)、高BMI (p=0.002)、腹部瘢痕(p=0.005)、可触及胆囊(p≤0.001)、胆囊壁厚(p≤0.001)、白细胞(p≤0.001)是预测腹腔镜胆囊切除术困难的重要因素。评分法易难截止点的灵敏度为72.6%,特异度为87.5%,ROC曲线下面积为0.849。评分方法难-极难截止点的灵敏度为70.0%,特异度为84.5%,ROC曲线下面积为0.779。结论:本研究评估的术前评分系统可靠,可用于预测腹腔镜胆囊切除术的难度。然而,需要进一步大样本量的随机前瞻性多中心研究来验证评分系统的有效性。
A Scoring System to Predict Difficult Laparoscopic Cholecystectomy: A Five-Year Cross-Sectional Study.
Background Laparoscopic cholecystectomy since long time already has become the preferred method because laparoscopic cholecystectomy has many advantages compared to standard open cholecystectomy. However, since it has associated with a higher risk of complication, preoperative prediction of risk factors is needed to assess the intraoperative difficulties. Various scoring systems have a role in predicting intraoperative difficulties; however, there is a need to find a consistent and reliable predictive system. Aim To validate a preoperative scoring system that will predict difficult laparoscopic cholecystectomy. Design of the Study. Nonrandomized retrospective descriptive study. Setting. Department of General Surgery, Lambung Mangkurat Univeristy Ulin Referral Hospital, Banjarmasin, Kalimantan Selatan, Indonesia. Methodology. A preoperative score was given to all the patients (134 patients from January 2015–December 2020) based on history, clinical examination, and sonographic findings. Using ROC curve, the cutoff for easy—difficult was 3.5 and difficult—very difficult was 7.5. The scores were compared in each patient to conclude the practicality of the preoperative predictive score. SPSS version 25 was used to analyze the data. Results History of hospitalization for acute cholecystitis (p ≤ 0.001), high BMI (p=0.002), abdominal scar (p=0.005), palpable gallbladder (p ≤ 0.001), thick gallbladder wall (p ≤ 0.001), and leucocyte (p ≤ 0.001) were considered as the significant factors that predict difficult laparoscopic cholecystectomy. Sensitivity and specificity for easy—difficult cutoff of the scoring method were 72.6% and 87.5%, respectively, with the area under the ROC curve being 0.849. Sensitivity and specificity for difficult—very difficult cutoff of the scoring method were 70.0% and 84.5%, respectively, with the area under the ROC curve being 0.779. Conclusion The preoperative scoring system evaluated in the study is reliable and beneficial in predicting the difficulty of laparoscopic cholecystectomy. However, further randomized prospective multicentric studies with large sample sizes are required to validate the efficiency of the scoring system.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
