Rajanshu Verma, Sanjaya K Satapathy, Muhammad Bilal
{"title":"降钙素原和c反应蛋白在自发性细菌性腹膜炎中的诊断价值。","authors":"Rajanshu Verma, Sanjaya K Satapathy, Muhammad Bilal","doi":"10.21037/tgh-19-297","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Spontaneous bacterial peritonitis (SBP) is a serious complication of cirrhosis and is associated with high morbidity and mortality. Rapid institution of appropriate antibiotics is central to the improved patient outcome. Correctly obtaining ascites fluid for analysis has several technical and logistic limitations resulting in overuse of empiric antibiotics when patients are admitted to the hospital with suspected SBP. Procalcitonin and C-reactive protein (CRP) are non-invasive markers of infection. We conducted a study to illustrate the role of these markers in making the diagnosis of SBP in patients with cirrhosis.</p><p><strong>Methods: </strong>A total of 45 patients were enrolled in this prospective cohort study, 14 (31.1%) of which were found to have SBP. Ascitic fluid neutrophils, serum procalcitonin and CRP levels were measured prior to initiation of antibiotics and these parameters were compared between the two groups. Area under receiver operator characteristic (AUROC) curves were used to assess the diagnostic accuracy of procalcitonin and CRP in this population. We defined neutrocytic SBP group as a combination of patients who had classic SBP (positive ascitic culture and >250 neutrophils/mm<sup>3</sup>) and culture-negative neutrocytic ascites.</p><p><strong>Results: </strong>Serum procalcitonin (2.81±2.59 <i>vs.</i> 0.43±0.48 ng/mL; P=0.0032), serum CRP (60.30±44.48 <i>vs.</i> 22.2±23.28; P=0.0055) and ascitic fluid neutrophil levels (49.23±30.90 <i>vs.</i> 16.7±20.39; P=0.0064) were significantly higher in SBP group than non-SBP group. AUROC for procalcitonin (cut-off >2.0 ng/mL) was 0.75 (95% CI, 0.61-0.88), CRP (cut-off >3.0 mg/L) was 0.55 (95% CI, 0.43-0.68) and for procalcitonin combined with CRP was 0.76 (95% CI, 0.61-0.90) for diagnosing all-cause SBP. In a subgroup analysis of patients with neutrocytic SBP, AUROC for procalcitonin was 0.88 (95% CI, 0.74-1.00), CRP was 0.62 (95% CI, 0.45-0.79) and for procalcitonin combined with CRP was 0.93 (95% CI, 0.81-1.00). Addition of CRP to procalcitonin did not significantly change the AUROC for diagnosis of SBP.</p><p><strong>Conclusions: </strong>Serum procalcitonin could be used as an adjunctive non-invasive biomarker in diagnosing SBP with a high degree of accuracy in cirrhotic patients. Addition of CRP does not seem to significantly increase the diagnostic accuracy of procalcitonin.</p>","PeriodicalId":23267,"journal":{"name":"Translational gastroenterology and hepatology","volume":" ","pages":"36"},"PeriodicalIF":3.0000,"publicationDate":"2022-10-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/6a/e5/tgh-07-19-297.PMC9468983.pdf","citationCount":"3","resultStr":"{\"title\":\"Procalcitonin and C-reactive protein in the diagnosis of spontaneous bacterial peritonitis.\",\"authors\":\"Rajanshu Verma, Sanjaya K Satapathy, Muhammad Bilal\",\"doi\":\"10.21037/tgh-19-297\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Spontaneous bacterial peritonitis (SBP) is a serious complication of cirrhosis and is associated with high morbidity and mortality. Rapid institution of appropriate antibiotics is central to the improved patient outcome. Correctly obtaining ascites fluid for analysis has several technical and logistic limitations resulting in overuse of empiric antibiotics when patients are admitted to the hospital with suspected SBP. Procalcitonin and C-reactive protein (CRP) are non-invasive markers of infection. We conducted a study to illustrate the role of these markers in making the diagnosis of SBP in patients with cirrhosis.</p><p><strong>Methods: </strong>A total of 45 patients were enrolled in this prospective cohort study, 14 (31.1%) of which were found to have SBP. Ascitic fluid neutrophils, serum procalcitonin and CRP levels were measured prior to initiation of antibiotics and these parameters were compared between the two groups. Area under receiver operator characteristic (AUROC) curves were used to assess the diagnostic accuracy of procalcitonin and CRP in this population. We defined neutrocytic SBP group as a combination of patients who had classic SBP (positive ascitic culture and >250 neutrophils/mm<sup>3</sup>) and culture-negative neutrocytic ascites.</p><p><strong>Results: </strong>Serum procalcitonin (2.81±2.59 <i>vs.</i> 0.43±0.48 ng/mL; P=0.0032), serum CRP (60.30±44.48 <i>vs.</i> 22.2±23.28; P=0.0055) and ascitic fluid neutrophil levels (49.23±30.90 <i>vs.</i> 16.7±20.39; P=0.0064) were significantly higher in SBP group than non-SBP group. AUROC for procalcitonin (cut-off >2.0 ng/mL) was 0.75 (95% CI, 0.61-0.88), CRP (cut-off >3.0 mg/L) was 0.55 (95% CI, 0.43-0.68) and for procalcitonin combined with CRP was 0.76 (95% CI, 0.61-0.90) for diagnosing all-cause SBP. In a subgroup analysis of patients with neutrocytic SBP, AUROC for procalcitonin was 0.88 (95% CI, 0.74-1.00), CRP was 0.62 (95% CI, 0.45-0.79) and for procalcitonin combined with CRP was 0.93 (95% CI, 0.81-1.00). Addition of CRP to procalcitonin did not significantly change the AUROC for diagnosis of SBP.</p><p><strong>Conclusions: </strong>Serum procalcitonin could be used as an adjunctive non-invasive biomarker in diagnosing SBP with a high degree of accuracy in cirrhotic patients. Addition of CRP does not seem to significantly increase the diagnostic accuracy of procalcitonin.</p>\",\"PeriodicalId\":23267,\"journal\":{\"name\":\"Translational gastroenterology and hepatology\",\"volume\":\" \",\"pages\":\"36\"},\"PeriodicalIF\":3.0000,\"publicationDate\":\"2022-10-25\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/6a/e5/tgh-07-19-297.PMC9468983.pdf\",\"citationCount\":\"3\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Translational gastroenterology and hepatology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.21037/tgh-19-297\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2022/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q1\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Translational gastroenterology and hepatology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.21037/tgh-19-297","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"Medicine","Score":null,"Total":0}
Procalcitonin and C-reactive protein in the diagnosis of spontaneous bacterial peritonitis.
Background: Spontaneous bacterial peritonitis (SBP) is a serious complication of cirrhosis and is associated with high morbidity and mortality. Rapid institution of appropriate antibiotics is central to the improved patient outcome. Correctly obtaining ascites fluid for analysis has several technical and logistic limitations resulting in overuse of empiric antibiotics when patients are admitted to the hospital with suspected SBP. Procalcitonin and C-reactive protein (CRP) are non-invasive markers of infection. We conducted a study to illustrate the role of these markers in making the diagnosis of SBP in patients with cirrhosis.
Methods: A total of 45 patients were enrolled in this prospective cohort study, 14 (31.1%) of which were found to have SBP. Ascitic fluid neutrophils, serum procalcitonin and CRP levels were measured prior to initiation of antibiotics and these parameters were compared between the two groups. Area under receiver operator characteristic (AUROC) curves were used to assess the diagnostic accuracy of procalcitonin and CRP in this population. We defined neutrocytic SBP group as a combination of patients who had classic SBP (positive ascitic culture and >250 neutrophils/mm3) and culture-negative neutrocytic ascites.
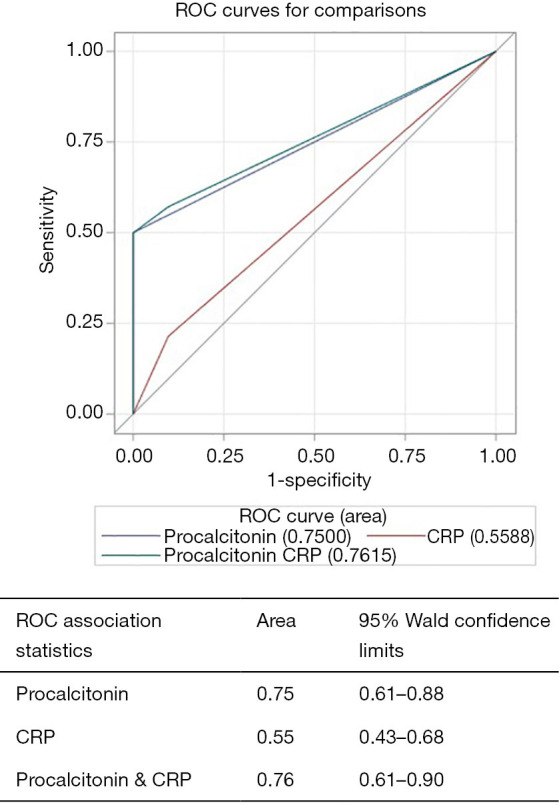
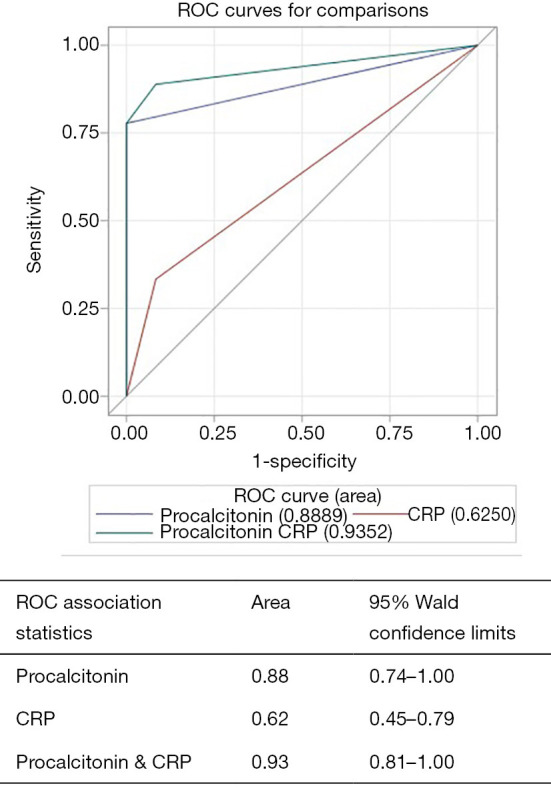
Results: Serum procalcitonin (2.81±2.59 vs. 0.43±0.48 ng/mL; P=0.0032), serum CRP (60.30±44.48 vs. 22.2±23.28; P=0.0055) and ascitic fluid neutrophil levels (49.23±30.90 vs. 16.7±20.39; P=0.0064) were significantly higher in SBP group than non-SBP group. AUROC for procalcitonin (cut-off >2.0 ng/mL) was 0.75 (95% CI, 0.61-0.88), CRP (cut-off >3.0 mg/L) was 0.55 (95% CI, 0.43-0.68) and for procalcitonin combined with CRP was 0.76 (95% CI, 0.61-0.90) for diagnosing all-cause SBP. In a subgroup analysis of patients with neutrocytic SBP, AUROC for procalcitonin was 0.88 (95% CI, 0.74-1.00), CRP was 0.62 (95% CI, 0.45-0.79) and for procalcitonin combined with CRP was 0.93 (95% CI, 0.81-1.00). Addition of CRP to procalcitonin did not significantly change the AUROC for diagnosis of SBP.
Conclusions: Serum procalcitonin could be used as an adjunctive non-invasive biomarker in diagnosing SBP with a high degree of accuracy in cirrhotic patients. Addition of CRP does not seem to significantly increase the diagnostic accuracy of procalcitonin.
期刊介绍:
Translational Gastroenterology and Hepatology (Transl Gastroenterol Hepatol; TGH; Online ISSN 2415-1289) is an open-access, peer-reviewed online journal that focuses on cutting-edge findings in the field of translational research in gastroenterology and hepatology and provides current and practical information on diagnosis, prevention and clinical investigations of gastrointestinal, pancreas, gallbladder and hepatic diseases. Specific areas of interest include, but not limited to, multimodality therapy, biomarkers, imaging, biology, pathology, and technical advances related to gastrointestinal and hepatic diseases. Contributions pertinent to gastroenterology and hepatology are also included from related fields such as nutrition, surgery, public health, human genetics, basic sciences, education, sociology, and nursing.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
