Senol Tonyali, Esteban Emiliani, Tarik Emre Şener, Amelia Pietropaolo, Mehmet Ӧzsoy, Omar Aboumarzouk, Bhaskar Somani, Panagiotis Kallidonis, Vincent M J De Coninck, Michele Talso, Etienne Xavier Keller, Nicola Macchione, Thomas Tailly
{"title":"泌尿科医师经皮肾镜取石术后临床不显著残余碎片的定义:EAU-YAU泌尿外科和尿石症工作组的一项全球调查。","authors":"Senol Tonyali, Esteban Emiliani, Tarik Emre Şener, Amelia Pietropaolo, Mehmet Ӧzsoy, Omar Aboumarzouk, Bhaskar Somani, Panagiotis Kallidonis, Vincent M J De Coninck, Michele Talso, Etienne Xavier Keller, Nicola Macchione, Thomas Tailly","doi":"10.5173/ceju.2022.0115","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>The aim of this article was to evaluate the current perception of urologists as to what size is considered as a clinically insignificant residual fragment (CIRF).</p><p><strong>Material and methods: </strong>A survey was globally distributed to the members of the Endourological Society via SurveyMonkey.</p><p><strong>Results: </strong>A total of 385 participants responded to the survey on CIRF. Most participants considered 2 mm (29%) as CIRF threshold, followed by 3 mm (24%), 4 mm (22%), 0 mm (14%), 5 mm (8%) and 1 mm (3%). North American urologists considered CIRF to be smaller than urologists from Asia, Eurasia and South America, (p-values ≤0.001, 0.037 and 0.015 respectively). European urologists identified smaller CIRF in comparison to Asian urologists (p-value = 0.001). Urologists mainly using a pneumatic lithotripter accepted larger fragments as CIRF, compared to urologists mainly using ultrasonic devices or a combination of ultrasonic and pneumatic devices (p-value = 0.026 and 0.005 respectively). Similarly, urologists mainly performing X-Ray and ultrasound as post-operative imaging accepted larger fragments as CIRF in comparison to urologists mainly performing non-contrast computed tomography (p-value = 0.001).</p><p><strong>Conclusions: </strong>What is considered as CIRF varies between urologist from different continents and seems to be associated with the lithotripter used and the post-operative imaging modality of preference to assess treatment success.</p>","PeriodicalId":9744,"journal":{"name":"Central European Journal of Urology","volume":"75 3","pages":"311-316"},"PeriodicalIF":1.9000,"publicationDate":"2022-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/ce/99/CEJU-75-0115.PMC9628728.pdf","citationCount":"1","resultStr":"{\"title\":\"Definition of clinically insignificant residual fragments after percutaneous nephrolithotomy among urologists: a world-wide survey by EAU-YAU Endourology and Urolithiasis Working Group.\",\"authors\":\"Senol Tonyali, Esteban Emiliani, Tarik Emre Şener, Amelia Pietropaolo, Mehmet Ӧzsoy, Omar Aboumarzouk, Bhaskar Somani, Panagiotis Kallidonis, Vincent M J De Coninck, Michele Talso, Etienne Xavier Keller, Nicola Macchione, Thomas Tailly\",\"doi\":\"10.5173/ceju.2022.0115\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>The aim of this article was to evaluate the current perception of urologists as to what size is considered as a clinically insignificant residual fragment (CIRF).</p><p><strong>Material and methods: </strong>A survey was globally distributed to the members of the Endourological Society via SurveyMonkey.</p><p><strong>Results: </strong>A total of 385 participants responded to the survey on CIRF. Most participants considered 2 mm (29%) as CIRF threshold, followed by 3 mm (24%), 4 mm (22%), 0 mm (14%), 5 mm (8%) and 1 mm (3%). North American urologists considered CIRF to be smaller than urologists from Asia, Eurasia and South America, (p-values ≤0.001, 0.037 and 0.015 respectively). European urologists identified smaller CIRF in comparison to Asian urologists (p-value = 0.001). Urologists mainly using a pneumatic lithotripter accepted larger fragments as CIRF, compared to urologists mainly using ultrasonic devices or a combination of ultrasonic and pneumatic devices (p-value = 0.026 and 0.005 respectively). Similarly, urologists mainly performing X-Ray and ultrasound as post-operative imaging accepted larger fragments as CIRF in comparison to urologists mainly performing non-contrast computed tomography (p-value = 0.001).</p><p><strong>Conclusions: </strong>What is considered as CIRF varies between urologist from different continents and seems to be associated with the lithotripter used and the post-operative imaging modality of preference to assess treatment success.</p>\",\"PeriodicalId\":9744,\"journal\":{\"name\":\"Central European Journal of Urology\",\"volume\":\"75 3\",\"pages\":\"311-316\"},\"PeriodicalIF\":1.9000,\"publicationDate\":\"2022-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/ce/99/CEJU-75-0115.PMC9628728.pdf\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Central European Journal of Urology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.5173/ceju.2022.0115\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2022/8/18 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"UROLOGY & NEPHROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Central European Journal of Urology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5173/ceju.2022.0115","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/8/18 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
Definition of clinically insignificant residual fragments after percutaneous nephrolithotomy among urologists: a world-wide survey by EAU-YAU Endourology and Urolithiasis Working Group.
Introduction: The aim of this article was to evaluate the current perception of urologists as to what size is considered as a clinically insignificant residual fragment (CIRF).
Material and methods: A survey was globally distributed to the members of the Endourological Society via SurveyMonkey.
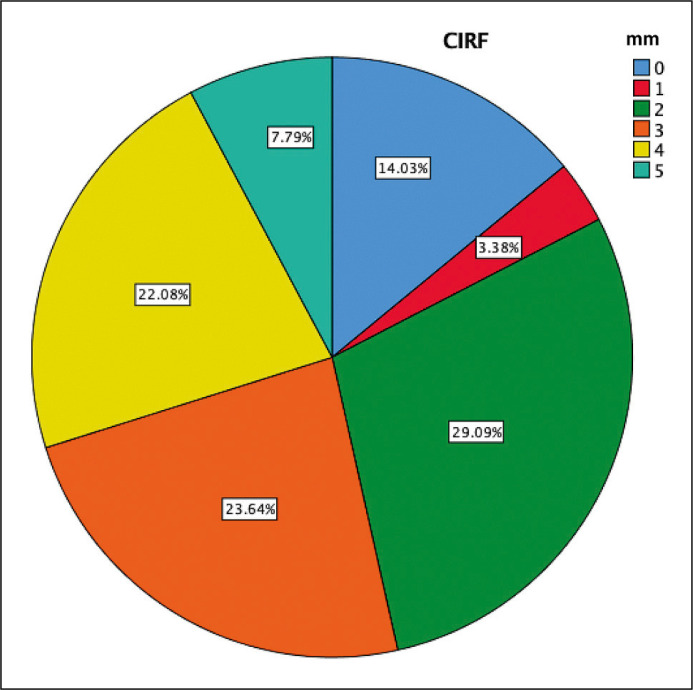
Results: A total of 385 participants responded to the survey on CIRF. Most participants considered 2 mm (29%) as CIRF threshold, followed by 3 mm (24%), 4 mm (22%), 0 mm (14%), 5 mm (8%) and 1 mm (3%). North American urologists considered CIRF to be smaller than urologists from Asia, Eurasia and South America, (p-values ≤0.001, 0.037 and 0.015 respectively). European urologists identified smaller CIRF in comparison to Asian urologists (p-value = 0.001). Urologists mainly using a pneumatic lithotripter accepted larger fragments as CIRF, compared to urologists mainly using ultrasonic devices or a combination of ultrasonic and pneumatic devices (p-value = 0.026 and 0.005 respectively). Similarly, urologists mainly performing X-Ray and ultrasound as post-operative imaging accepted larger fragments as CIRF in comparison to urologists mainly performing non-contrast computed tomography (p-value = 0.001).
Conclusions: What is considered as CIRF varies between urologist from different continents and seems to be associated with the lithotripter used and the post-operative imaging modality of preference to assess treatment success.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
