Joao Leote, Tiago Judas, Ana Luísa Broa, Miguel Lopes, Francisca Abecasis, Inês Pintassilgo, Afonso Gonçalves, Filipe Gonzalez
{"title":"新型冠状病毒肺炎合并心功能障碍患者肺部超声表现的时间过程分析。","authors":"Joao Leote, Tiago Judas, Ana Luísa Broa, Miguel Lopes, Francisca Abecasis, Inês Pintassilgo, Afonso Gonçalves, Filipe Gonzalez","doi":"10.1186/s13089-022-00278-2","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Lung ultrasound (LUS) is a valuable tool to predict and monitor the COVID-19 pneumonia course. However, the influence of cardiac dysfunction (CD) on LUS findings remains to be studied. Our objective was to determine the effect of CD on LUS in hospitalized patients with COVID-19 pneumonia.</p><p><strong>Material and methods: </strong>Fifty-one patients with COVID-19 pneumonia participated in the study. Focused echocardiography (FoCUS) was carried out on day 1 to separate patients into two groups depending on whether they had FoCUS signs of CD (CD+ vs CD-). LUS scores, based on the thickness of the pleural line, the B-line characteristics, and the presence or not of consolidations, were obtained three times along the patient's admission (D1, D5, D10) and compared between CD+ and CD- patients. A correlation analysis was carried out between LUS scores and the ratio of the arterial partial pressure of oxygen to the fraction of the inspired oxygen (P/F ratio).</p><p><strong>Results: </strong>Twenty-two patients were CD+ and 29 patients were CD-. Among the CD+ patients, 19 were admitted to the intensive care unit (ICU), seven received invasive mechanical ventilation (IMV), and one did not survive. Among the CD- patients, 11 were admitted to the ICU, one received IMV and seven did not survive. CD+ patients showed a significantly lower P/F ratio than CD- patients. However, LUS scores showed no between-group differences, except for fewer subpleural consolidations in the upper quadrants of CD+ than on CD- patients.</p><p><strong>Conclusion: </strong>In patients with COVID-19, CD contributed to a worse clinical course, but it did not induce significant changes in LUS. Our findings suggest that pathophysiological factors other than those reflected by LUS may be responsible for the differences in clinical condition between CD+ and CD- patients.</p>","PeriodicalId":36911,"journal":{"name":"Ultrasound Journal","volume":" ","pages":"28"},"PeriodicalIF":2.9000,"publicationDate":"2022-07-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9261145/pdf/","citationCount":"3","resultStr":"{\"title\":\"Time course of lung ultrasound findings in patients with COVID-19 pneumonia and cardiac dysfunction.\",\"authors\":\"Joao Leote, Tiago Judas, Ana Luísa Broa, Miguel Lopes, Francisca Abecasis, Inês Pintassilgo, Afonso Gonçalves, Filipe Gonzalez\",\"doi\":\"10.1186/s13089-022-00278-2\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Lung ultrasound (LUS) is a valuable tool to predict and monitor the COVID-19 pneumonia course. However, the influence of cardiac dysfunction (CD) on LUS findings remains to be studied. Our objective was to determine the effect of CD on LUS in hospitalized patients with COVID-19 pneumonia.</p><p><strong>Material and methods: </strong>Fifty-one patients with COVID-19 pneumonia participated in the study. Focused echocardiography (FoCUS) was carried out on day 1 to separate patients into two groups depending on whether they had FoCUS signs of CD (CD+ vs CD-). LUS scores, based on the thickness of the pleural line, the B-line characteristics, and the presence or not of consolidations, were obtained three times along the patient's admission (D1, D5, D10) and compared between CD+ and CD- patients. A correlation analysis was carried out between LUS scores and the ratio of the arterial partial pressure of oxygen to the fraction of the inspired oxygen (P/F ratio).</p><p><strong>Results: </strong>Twenty-two patients were CD+ and 29 patients were CD-. Among the CD+ patients, 19 were admitted to the intensive care unit (ICU), seven received invasive mechanical ventilation (IMV), and one did not survive. Among the CD- patients, 11 were admitted to the ICU, one received IMV and seven did not survive. CD+ patients showed a significantly lower P/F ratio than CD- patients. However, LUS scores showed no between-group differences, except for fewer subpleural consolidations in the upper quadrants of CD+ than on CD- patients.</p><p><strong>Conclusion: </strong>In patients with COVID-19, CD contributed to a worse clinical course, but it did not induce significant changes in LUS. Our findings suggest that pathophysiological factors other than those reflected by LUS may be responsible for the differences in clinical condition between CD+ and CD- patients.</p>\",\"PeriodicalId\":36911,\"journal\":{\"name\":\"Ultrasound Journal\",\"volume\":\" \",\"pages\":\"28\"},\"PeriodicalIF\":2.9000,\"publicationDate\":\"2022-07-07\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9261145/pdf/\",\"citationCount\":\"3\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Ultrasound Journal\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s13089-022-00278-2\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Ultrasound Journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s13089-022-00278-2","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 3
摘要
背景:肺超声(LUS)是预测和监测COVID-19肺炎病程的重要工具。然而,心功能障碍(CD)对LUS结果的影响仍有待研究。我们的目的是确定CD对COVID-19肺炎住院患者LUS的影响。材料与方法:51例新冠肺炎患者参与研究。第1天进行焦点超声心动图(FoCUS),根据患者是否有CD的焦点征象(CD+ vs CD-)将患者分为两组。根据胸膜线厚度、b线特征和有无实变,在患者入院时获得三次LUS评分(D1、D5、D10),并比较CD+和CD-患者的LUS评分。将LUS评分与动脉血氧分压与吸入氧分数之比(P/F ratio)进行相关性分析。结果:CD+ 22例,CD- 29例。在CD+患者中,19人入住重症监护病房(ICU), 7人接受有创机械通气(IMV), 1人死亡。在CD患者中,11人住进ICU, 1人接受IMV治疗,7人死亡。CD+患者P/F比值明显低于CD-患者。然而,LUS评分没有显示组间差异,除了CD+患者的胸膜下实变少于CD-患者。结论:在COVID-19患者中,CD加重了临床病程,但未引起LUS的显著变化。我们的研究结果表明,LUS所反映的病理生理因素之外的其他因素可能是导致CD+和CD-患者临床状况差异的原因。
Time course of lung ultrasound findings in patients with COVID-19 pneumonia and cardiac dysfunction.
Background: Lung ultrasound (LUS) is a valuable tool to predict and monitor the COVID-19 pneumonia course. However, the influence of cardiac dysfunction (CD) on LUS findings remains to be studied. Our objective was to determine the effect of CD on LUS in hospitalized patients with COVID-19 pneumonia.
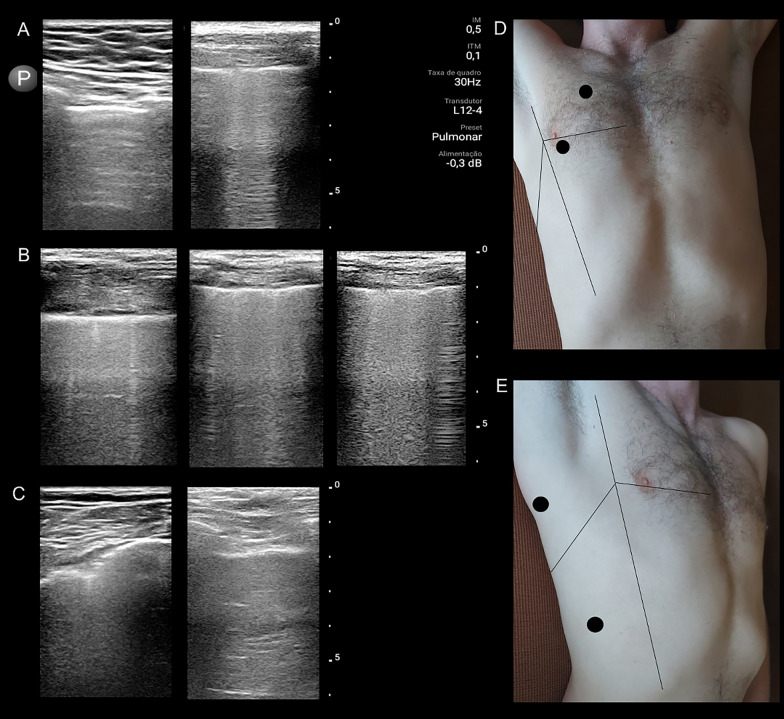
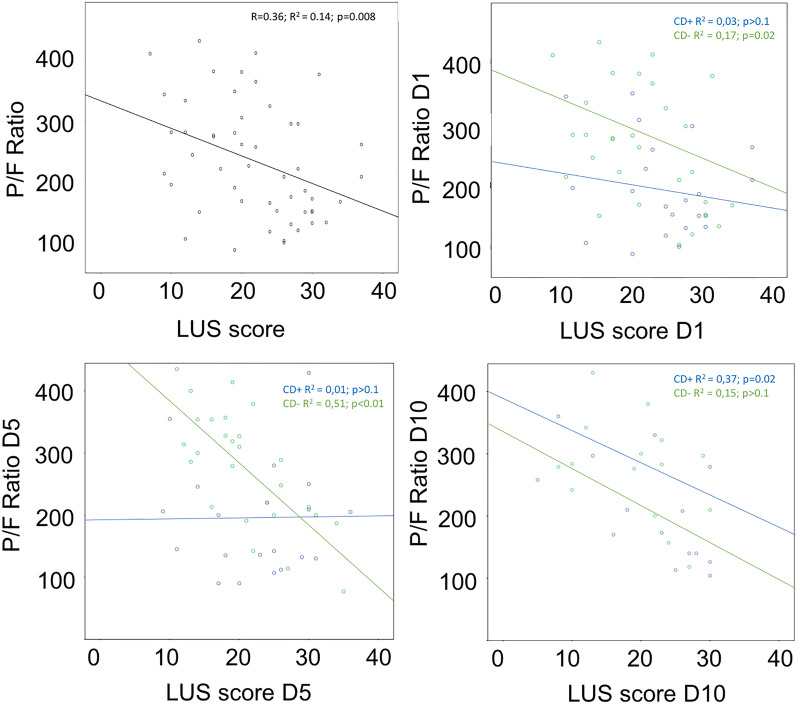
Material and methods: Fifty-one patients with COVID-19 pneumonia participated in the study. Focused echocardiography (FoCUS) was carried out on day 1 to separate patients into two groups depending on whether they had FoCUS signs of CD (CD+ vs CD-). LUS scores, based on the thickness of the pleural line, the B-line characteristics, and the presence or not of consolidations, were obtained three times along the patient's admission (D1, D5, D10) and compared between CD+ and CD- patients. A correlation analysis was carried out between LUS scores and the ratio of the arterial partial pressure of oxygen to the fraction of the inspired oxygen (P/F ratio).
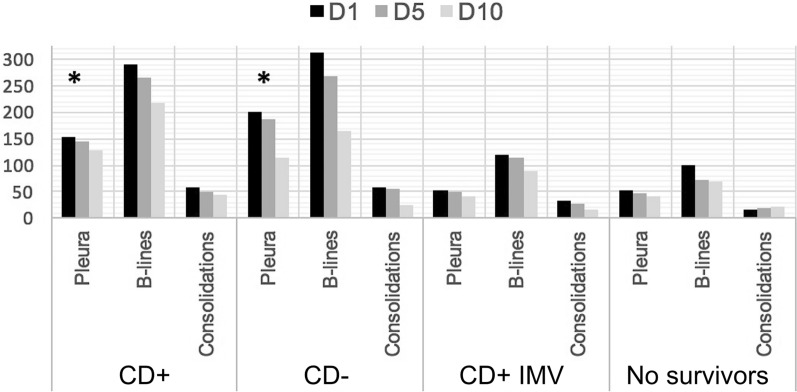
Results: Twenty-two patients were CD+ and 29 patients were CD-. Among the CD+ patients, 19 were admitted to the intensive care unit (ICU), seven received invasive mechanical ventilation (IMV), and one did not survive. Among the CD- patients, 11 were admitted to the ICU, one received IMV and seven did not survive. CD+ patients showed a significantly lower P/F ratio than CD- patients. However, LUS scores showed no between-group differences, except for fewer subpleural consolidations in the upper quadrants of CD+ than on CD- patients.
Conclusion: In patients with COVID-19, CD contributed to a worse clinical course, but it did not induce significant changes in LUS. Our findings suggest that pathophysiological factors other than those reflected by LUS may be responsible for the differences in clinical condition between CD+ and CD- patients.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
