Smit Patel, Scott Dickinson, Kevin Morris, Helen F Ashdown, James D Chalmers
{"title":"COPD患者吸入皮质类固醇停药的描述性队列研究。","authors":"Smit Patel, Scott Dickinson, Kevin Morris, Helen F Ashdown, James D Chalmers","doi":"10.1038/s41533-022-00288-6","DOIUrl":null,"url":null,"abstract":"<p><p>Inhaled corticosteroid (ICS) therapy is widely prescribed without a history of exacerbations and consensus guidelines suggest withdrawal of ICS in these patients would reduce the risk of side effects and promote cost-effective prescribing. The study describes the prescribing behaviour in the United Kingdom (UK) in relation to ICS withdrawal and identifies clinical outcomes following withdrawal using primary and secondary care electronic health records between January 2012 and December 2017. Patients with a history ≥12 months' exposure who withdrew ICS for ≥6 months were identified into two cohorts; those prescribed a long-acting bronchodilator maintenance therapy and those that were not prescribed any maintenance therapy. The duration of withdrawal, predictors of restarting ICS, and clinical outcomes were compared between both patient cohorts. Among 76,808 patients that had ≥1 prescription of ICS in the study period, 11,093 patients (14%) withdrew ICS therapy at least once during the study period. The median time without ICS was 9 months (IQR 7-14), with the majority (71%) receiving subsequent ICS prescriptions after withdrawal. Patients receiving maintenance therapy with a COPD review at withdrawal were 28% less likely to restart ICS (HR: 0.72, 95% CI 0.61, 0.85). Overall, 69% and 89% of patients that withdrew ICS had no recorded exacerbation event or COPD hospitalisation, respectively, during the withdrawal. This study provides evidence that most patients withdrawing from ICS do not experience COPD exacerbations and withdrawal success can be achieved by carefully planning routine COPD reviews whilst optimising the use of available maintenance therapies.</p>","PeriodicalId":19470,"journal":{"name":"NPJ Primary Care Respiratory Medicine","volume":null,"pages":null},"PeriodicalIF":3.1000,"publicationDate":"2022-07-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9300648/pdf/","citationCount":"2","resultStr":"{\"title\":\"A descriptive cohort study of withdrawal from inhaled corticosteroids in COPD patients.\",\"authors\":\"Smit Patel, Scott Dickinson, Kevin Morris, Helen F Ashdown, James D Chalmers\",\"doi\":\"10.1038/s41533-022-00288-6\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Inhaled corticosteroid (ICS) therapy is widely prescribed without a history of exacerbations and consensus guidelines suggest withdrawal of ICS in these patients would reduce the risk of side effects and promote cost-effective prescribing. The study describes the prescribing behaviour in the United Kingdom (UK) in relation to ICS withdrawal and identifies clinical outcomes following withdrawal using primary and secondary care electronic health records between January 2012 and December 2017. Patients with a history ≥12 months' exposure who withdrew ICS for ≥6 months were identified into two cohorts; those prescribed a long-acting bronchodilator maintenance therapy and those that were not prescribed any maintenance therapy. The duration of withdrawal, predictors of restarting ICS, and clinical outcomes were compared between both patient cohorts. Among 76,808 patients that had ≥1 prescription of ICS in the study period, 11,093 patients (14%) withdrew ICS therapy at least once during the study period. The median time without ICS was 9 months (IQR 7-14), with the majority (71%) receiving subsequent ICS prescriptions after withdrawal. Patients receiving maintenance therapy with a COPD review at withdrawal were 28% less likely to restart ICS (HR: 0.72, 95% CI 0.61, 0.85). Overall, 69% and 89% of patients that withdrew ICS had no recorded exacerbation event or COPD hospitalisation, respectively, during the withdrawal. This study provides evidence that most patients withdrawing from ICS do not experience COPD exacerbations and withdrawal success can be achieved by carefully planning routine COPD reviews whilst optimising the use of available maintenance therapies.</p>\",\"PeriodicalId\":19470,\"journal\":{\"name\":\"NPJ Primary Care Respiratory Medicine\",\"volume\":null,\"pages\":null},\"PeriodicalIF\":3.1000,\"publicationDate\":\"2022-07-20\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9300648/pdf/\",\"citationCount\":\"2\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"NPJ Primary Care Respiratory Medicine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1038/s41533-022-00288-6\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"PRIMARY HEALTH CARE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"NPJ Primary Care Respiratory Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1038/s41533-022-00288-6","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"PRIMARY HEALTH CARE","Score":null,"Total":0}
引用次数: 2
摘要
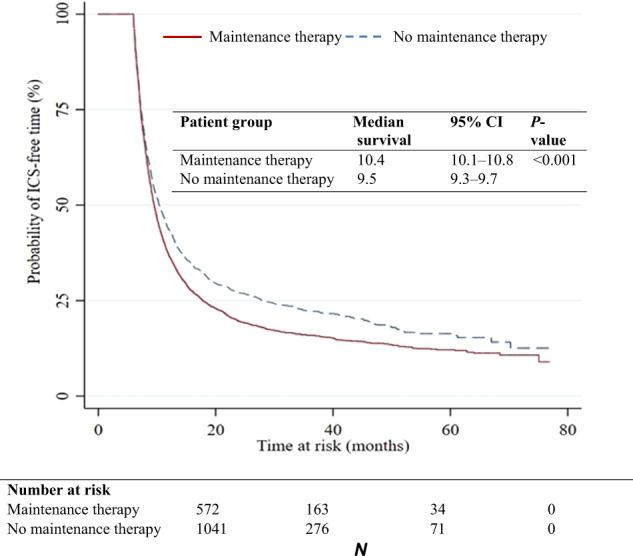
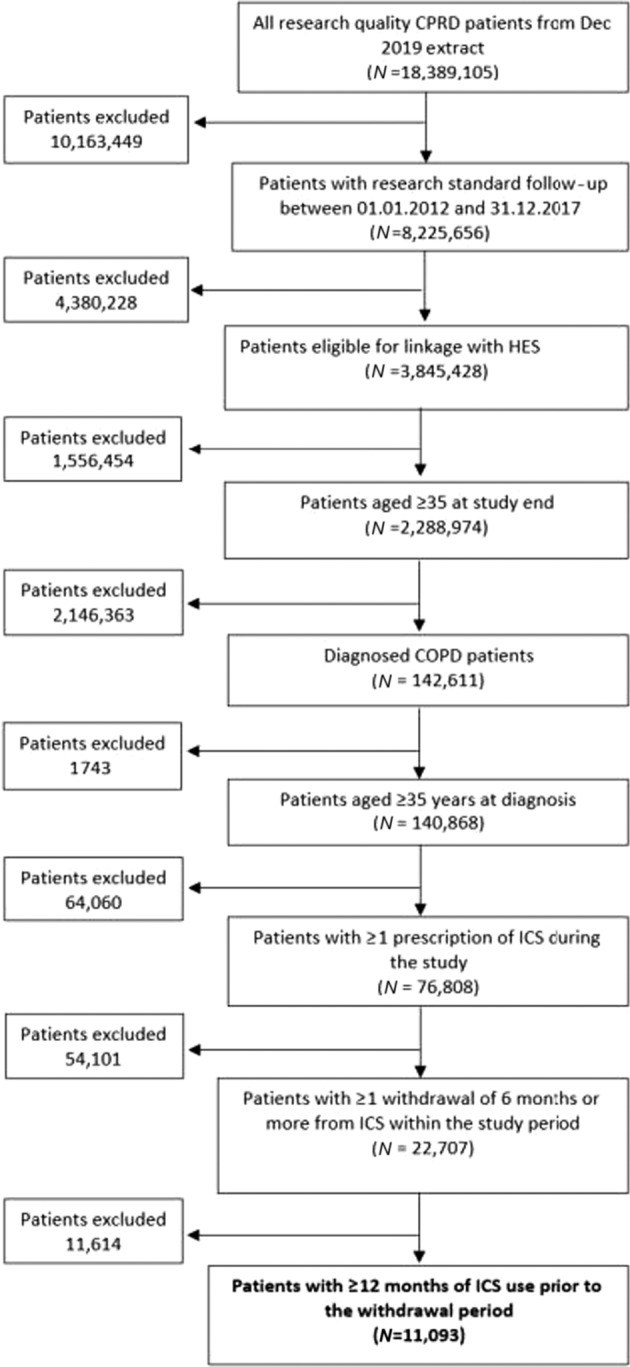
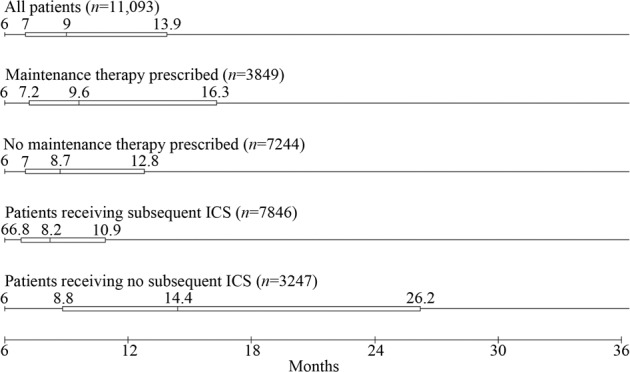
吸入皮质类固醇(ICS)治疗在没有病情加重史的情况下被广泛使用,共识指南建议,在这些患者中停用ICS可以降低副作用的风险,并促进具有成本效益的处方。该研究描述了英国(UK)与ICS戒断相关的处方行为,并确定了2012年1月至2017年12月期间使用初级和二级保健电子健康记录戒断后的临床结果。暴露史≥12个月且停药≥6个月的患者被分为两组;一组使用长效支气管扩张剂维持治疗另一组没有使用任何维持治疗。对两组患者的停药时间、重新启动ICS的预测因素和临床结果进行比较。在研究期间服用ICS处方≥1次的76,808例患者中,11093例(14%)患者在研究期间至少停药一次。未使用ICS的中位时间为9个月(IQR 7-14),大多数(71%)患者在停药后继续使用ICS处方。接受维持治疗并在停药时复查COPD的患者重启ICS的可能性降低28% (HR: 0.72, 95% CI 0.61, 0.85)。总体而言,69%和89%的停药ICS患者在停药期间分别没有记录的加重事件或COPD住院。该研究提供的证据表明,大多数退出ICS的患者没有经历COPD恶化,并且通过仔细规划常规COPD审查,同时优化现有维持疗法的使用,可以实现成功的退出。
A descriptive cohort study of withdrawal from inhaled corticosteroids in COPD patients.
Inhaled corticosteroid (ICS) therapy is widely prescribed without a history of exacerbations and consensus guidelines suggest withdrawal of ICS in these patients would reduce the risk of side effects and promote cost-effective prescribing. The study describes the prescribing behaviour in the United Kingdom (UK) in relation to ICS withdrawal and identifies clinical outcomes following withdrawal using primary and secondary care electronic health records between January 2012 and December 2017. Patients with a history ≥12 months' exposure who withdrew ICS for ≥6 months were identified into two cohorts; those prescribed a long-acting bronchodilator maintenance therapy and those that were not prescribed any maintenance therapy. The duration of withdrawal, predictors of restarting ICS, and clinical outcomes were compared between both patient cohorts. Among 76,808 patients that had ≥1 prescription of ICS in the study period, 11,093 patients (14%) withdrew ICS therapy at least once during the study period. The median time without ICS was 9 months (IQR 7-14), with the majority (71%) receiving subsequent ICS prescriptions after withdrawal. Patients receiving maintenance therapy with a COPD review at withdrawal were 28% less likely to restart ICS (HR: 0.72, 95% CI 0.61, 0.85). Overall, 69% and 89% of patients that withdrew ICS had no recorded exacerbation event or COPD hospitalisation, respectively, during the withdrawal. This study provides evidence that most patients withdrawing from ICS do not experience COPD exacerbations and withdrawal success can be achieved by carefully planning routine COPD reviews whilst optimising the use of available maintenance therapies.
期刊介绍:
npj Primary Care Respiratory Medicine is an open access, online-only, multidisciplinary journal dedicated to publishing high-quality research in all areas of the primary care management of respiratory and respiratory-related allergic diseases. Papers published by the journal represent important advances of significance to specialists within the fields of primary care and respiratory medicine. We are particularly interested in receiving papers in relation to the following aspects of respiratory medicine, respiratory-related allergic diseases and tobacco control:
epidemiology
prevention
clinical care
service delivery and organisation of healthcare (including implementation science)
global health.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
