Qing Ye, Yichen Zhao, Kemin Liu, Cheng Zhao, Yang Liu, Yuqi Li, Jiangang Wang
{"title":"伴有或不伴有巨大左心房的二尖瓣手术患者的射频消融。","authors":"Qing Ye, Yichen Zhao, Kemin Liu, Cheng Zhao, Yang Liu, Yuqi Li, Jiangang Wang","doi":"10.5761/atcs.oa.22-00033","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>We aimed to compare the efficacy of radiofrequency ablation (RFA) in patients undergoing mitral valve (MV) surgery with or without giant left atria.</p><p><strong>Methods: </strong>This retrospective, single-center, cohort study investigated patients who underwent MV surgery and concomitant RFA from 2009 to 2019. Patients were divided into non-giant left atria (diameter ≤65 mm, n = 1543) and giant left atria (diameter >65 mm, n = 241) groups. Five-year freedom from atrial tachyarrhythmia recurrence and thromboembolic event (TE) rates were assessed with death as the competing risk factor with and without propensity-score matching.</p><p><strong>Results: </strong>Patients with giant left atria had higher mortality (10.8% versus 6.2%, P = 0.008) and readmission rates for heart failure than those without (12.0% versus 6.8%, P = 0.004). Atrial tachyarrhythmia recurrence rates were higher in patients with giant left atria than in those without (49% versus 24% at 5 years, P <0.001), but the cumulative incidence of TEs before (P = 0.944) and after (P = 0.695) propensity-score matching was comparable.</p><p><strong>Conclusions: </strong>RFA effectively prevented TEs in patients with giant left atria, despite significant atrial tachyarrhythmia recurrence. Atrial tachyarrhythmia recurrence did not increase the risk of TEs. A lower success rate should be considered when deciding whether to perform surgical ablation in patients with giant left atria.</p>","PeriodicalId":93877,"journal":{"name":"Annals of thoracic and cardiovascular surgery : official journal of the Association of Thoracic and Cardiovascular Surgeons of Asia","volume":" ","pages":"349-358"},"PeriodicalIF":1.3000,"publicationDate":"2022-10-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/90/80/atcs-28-349.PMC9585334.pdf","citationCount":"1","resultStr":"{\"title\":\"Radiofrequency Ablation in Patients Undergoing Mitral Valve Surgery with or without Giant Left Atria.\",\"authors\":\"Qing Ye, Yichen Zhao, Kemin Liu, Cheng Zhao, Yang Liu, Yuqi Li, Jiangang Wang\",\"doi\":\"10.5761/atcs.oa.22-00033\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Purpose: </strong>We aimed to compare the efficacy of radiofrequency ablation (RFA) in patients undergoing mitral valve (MV) surgery with or without giant left atria.</p><p><strong>Methods: </strong>This retrospective, single-center, cohort study investigated patients who underwent MV surgery and concomitant RFA from 2009 to 2019. Patients were divided into non-giant left atria (diameter ≤65 mm, n = 1543) and giant left atria (diameter >65 mm, n = 241) groups. Five-year freedom from atrial tachyarrhythmia recurrence and thromboembolic event (TE) rates were assessed with death as the competing risk factor with and without propensity-score matching.</p><p><strong>Results: </strong>Patients with giant left atria had higher mortality (10.8% versus 6.2%, P = 0.008) and readmission rates for heart failure than those without (12.0% versus 6.8%, P = 0.004). Atrial tachyarrhythmia recurrence rates were higher in patients with giant left atria than in those without (49% versus 24% at 5 years, P <0.001), but the cumulative incidence of TEs before (P = 0.944) and after (P = 0.695) propensity-score matching was comparable.</p><p><strong>Conclusions: </strong>RFA effectively prevented TEs in patients with giant left atria, despite significant atrial tachyarrhythmia recurrence. Atrial tachyarrhythmia recurrence did not increase the risk of TEs. A lower success rate should be considered when deciding whether to perform surgical ablation in patients with giant left atria.</p>\",\"PeriodicalId\":93877,\"journal\":{\"name\":\"Annals of thoracic and cardiovascular surgery : official journal of the Association of Thoracic and Cardiovascular Surgeons of Asia\",\"volume\":\" \",\"pages\":\"349-358\"},\"PeriodicalIF\":1.3000,\"publicationDate\":\"2022-10-20\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/90/80/atcs-28-349.PMC9585334.pdf\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Annals of thoracic and cardiovascular surgery : official journal of the Association of Thoracic and Cardiovascular Surgeons of Asia\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.5761/atcs.oa.22-00033\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2022/7/6 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of thoracic and cardiovascular surgery : official journal of the Association of Thoracic and Cardiovascular Surgeons of Asia","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.5761/atcs.oa.22-00033","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/7/6 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 1
摘要
目的:我们的目的是比较射频消融(RFA)在二尖瓣(MV)手术患者有或没有巨大左心房的疗效。方法:这项回顾性、单中心、队列研究调查了2009年至2019年接受MV手术并合并RFA的患者。患者分为左心房非巨幅组(直径≤65 mm, n = 1543)和左心房巨幅组(直径>65 mm, n = 241)。5年无房性心动过速复发和血栓栓塞事件(TE)发生率的评估以死亡作为竞争风险因素,有和没有倾向评分匹配。结果:巨大左心房患者的死亡率(10.8%比6.2%,P = 0.008)和心力衰竭再入院率(12.0%比6.8%,P = 0.004)高于无巨大左心房患者。有巨大左心房的患者的房性心动过速复发率高于无巨大左心房的患者(5年时分别为49%和24%)。结论:尽管有显著的房性心动过速复发率,但RFA有效地预防了巨大左心房患者的TEs。心房速性心律失常复发不增加TEs发生的风险。在决定是否对巨大左心房进行手术消融时应考虑较低的成功率。
Radiofrequency Ablation in Patients Undergoing Mitral Valve Surgery with or without Giant Left Atria.
Purpose: We aimed to compare the efficacy of radiofrequency ablation (RFA) in patients undergoing mitral valve (MV) surgery with or without giant left atria.
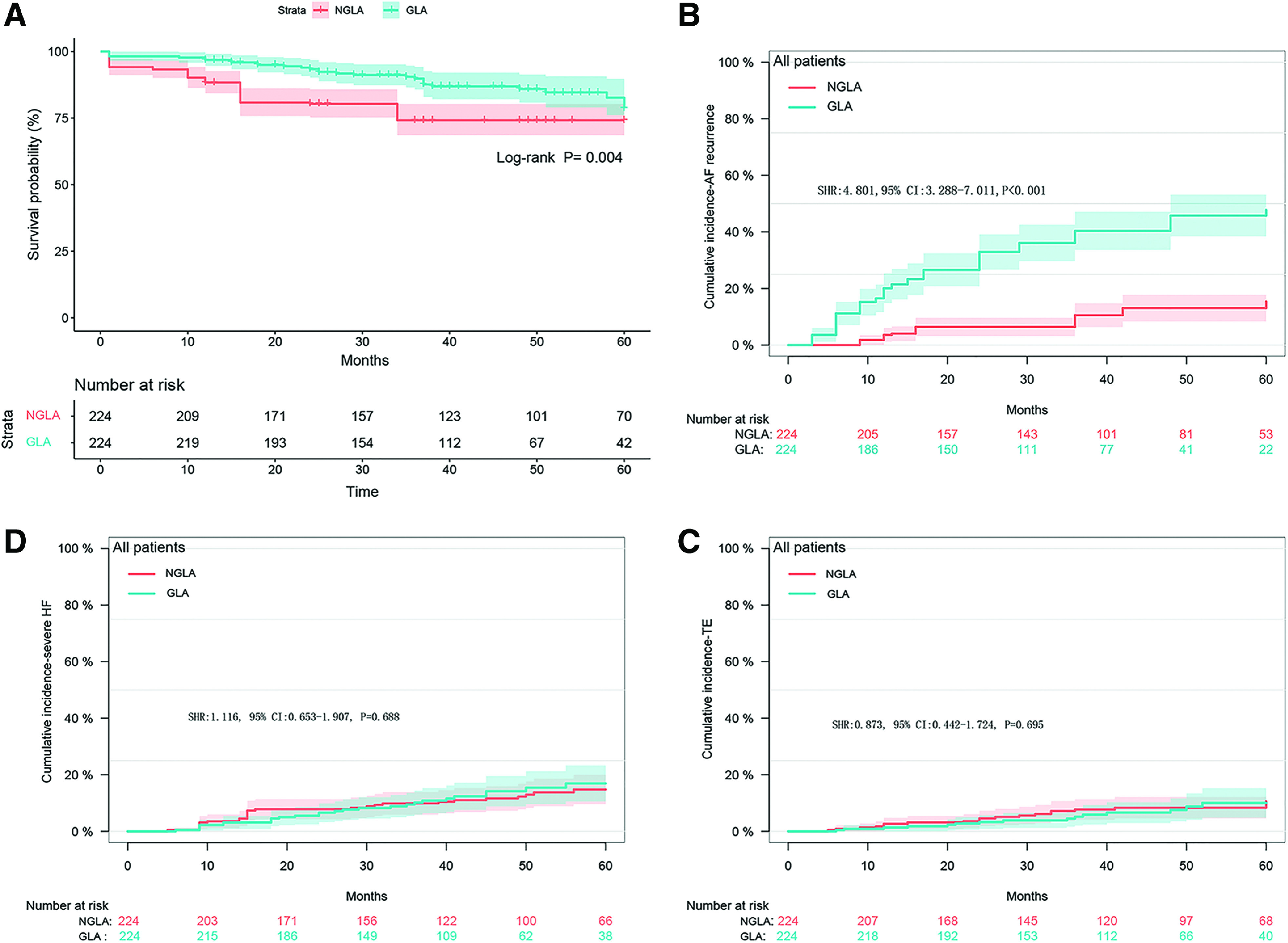
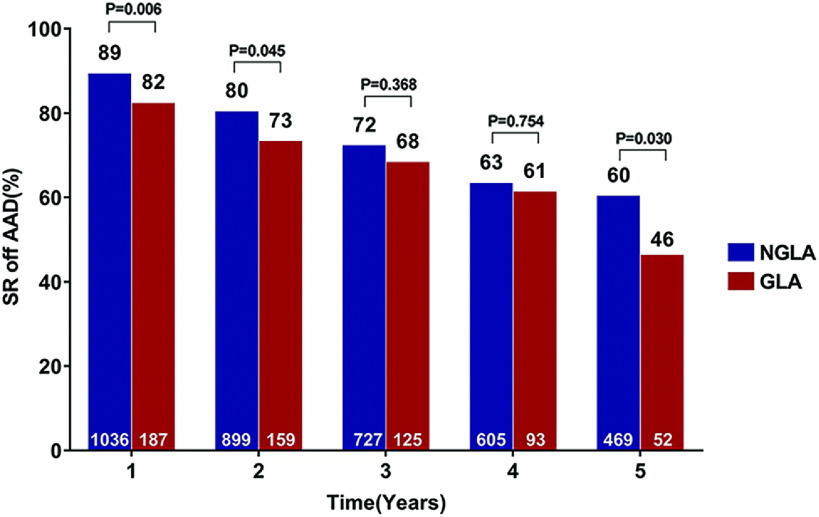
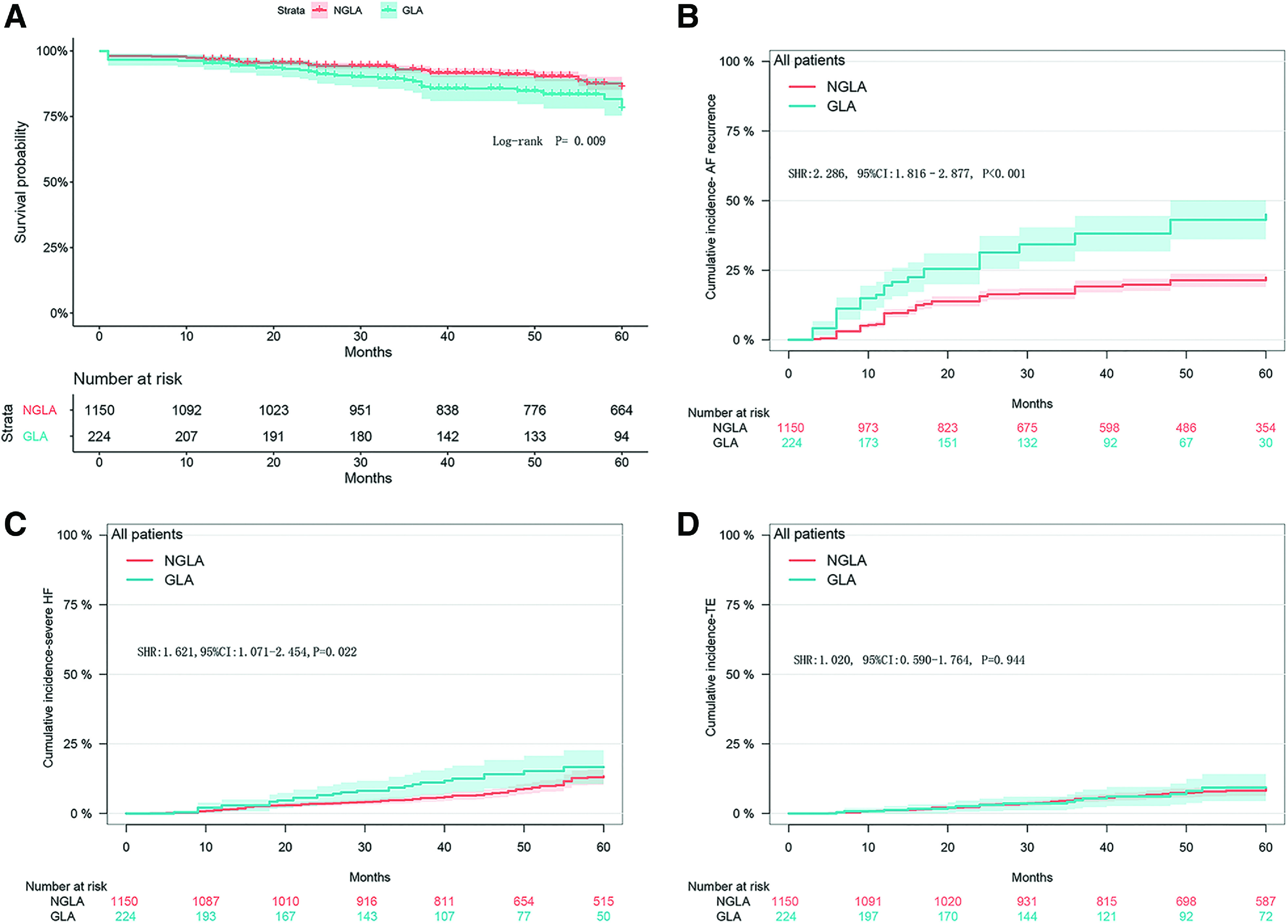
Methods: This retrospective, single-center, cohort study investigated patients who underwent MV surgery and concomitant RFA from 2009 to 2019. Patients were divided into non-giant left atria (diameter ≤65 mm, n = 1543) and giant left atria (diameter >65 mm, n = 241) groups. Five-year freedom from atrial tachyarrhythmia recurrence and thromboembolic event (TE) rates were assessed with death as the competing risk factor with and without propensity-score matching.
Results: Patients with giant left atria had higher mortality (10.8% versus 6.2%, P = 0.008) and readmission rates for heart failure than those without (12.0% versus 6.8%, P = 0.004). Atrial tachyarrhythmia recurrence rates were higher in patients with giant left atria than in those without (49% versus 24% at 5 years, P <0.001), but the cumulative incidence of TEs before (P = 0.944) and after (P = 0.695) propensity-score matching was comparable.
Conclusions: RFA effectively prevented TEs in patients with giant left atria, despite significant atrial tachyarrhythmia recurrence. Atrial tachyarrhythmia recurrence did not increase the risk of TEs. A lower success rate should be considered when deciding whether to perform surgical ablation in patients with giant left atria.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
