{"title":"梗阻性肥厚性肌病二尖瓣收缩前运动(SAM)的外科治疗。","authors":"Akihiko Usui, Masato Mutsuga","doi":"10.5761/atcs.ra.22-00103","DOIUrl":null,"url":null,"abstract":"<p><p>In patients with obstructive hypertrophic cardiomyopathy, left ventricular outflow tract (LVOT) obstruction can be created by the hypertrophic interventricular septum (IVS) as well as systolic anterior motion (SAM) of the anterior mitral leaflet (AML). Sufficient septal myectomy is a fundamental surgical technique to treat LVOT obstruction, however, direct surgical management for SAM is another key aspect. Besides the hypertrophic IVS, mitral valve, subvalvular apparatus, and papillary muscle may play important role for SAM and several surgical techniques have been proposed to treat SAM in literature. In this review, each surgical technique is classified by the anatomical structure on which the surgical procedure is applied. The AML is the main surgical site and is applied with plication (vertical plication, resection-plication-release strategy), extension (the AML extension, transverse incision of the AML), sutured (edge-to-edge repair, anterior leaflet retention plasty), or traction (floating stitch, papillary muscle-to-anterior annulus stitches, paradoxical stitches, transposition of a directed chorda tendinea to the AML). Height reduction of the posterior mitral valve leaflet and papillary muscle reorientation are other techniques. We should understand theoretical aspects of each technique on correction of anatomical and functional abnormalities of the structure and should apply them under proper indication.</p>","PeriodicalId":93877,"journal":{"name":"Annals of thoracic and cardiovascular surgery : official journal of the Association of Thoracic and Cardiovascular Surgeons of Asia","volume":" ","pages":"239-248"},"PeriodicalIF":1.3000,"publicationDate":"2022-08-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/91/fa/atcs-28-239.PMC9433892.pdf","citationCount":"2","resultStr":"{\"title\":\"Surgical Management for Systolic Anterior Motion (SAM) of the Mitral Valve in Obstructive Hypertrophic Myopathy.\",\"authors\":\"Akihiko Usui, Masato Mutsuga\",\"doi\":\"10.5761/atcs.ra.22-00103\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>In patients with obstructive hypertrophic cardiomyopathy, left ventricular outflow tract (LVOT) obstruction can be created by the hypertrophic interventricular septum (IVS) as well as systolic anterior motion (SAM) of the anterior mitral leaflet (AML). Sufficient septal myectomy is a fundamental surgical technique to treat LVOT obstruction, however, direct surgical management for SAM is another key aspect. Besides the hypertrophic IVS, mitral valve, subvalvular apparatus, and papillary muscle may play important role for SAM and several surgical techniques have been proposed to treat SAM in literature. In this review, each surgical technique is classified by the anatomical structure on which the surgical procedure is applied. The AML is the main surgical site and is applied with plication (vertical plication, resection-plication-release strategy), extension (the AML extension, transverse incision of the AML), sutured (edge-to-edge repair, anterior leaflet retention plasty), or traction (floating stitch, papillary muscle-to-anterior annulus stitches, paradoxical stitches, transposition of a directed chorda tendinea to the AML). Height reduction of the posterior mitral valve leaflet and papillary muscle reorientation are other techniques. We should understand theoretical aspects of each technique on correction of anatomical and functional abnormalities of the structure and should apply them under proper indication.</p>\",\"PeriodicalId\":93877,\"journal\":{\"name\":\"Annals of thoracic and cardiovascular surgery : official journal of the Association of Thoracic and Cardiovascular Surgeons of Asia\",\"volume\":\" \",\"pages\":\"239-248\"},\"PeriodicalIF\":1.3000,\"publicationDate\":\"2022-08-20\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/91/fa/atcs-28-239.PMC9433892.pdf\",\"citationCount\":\"2\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Annals of thoracic and cardiovascular surgery : official journal of the Association of Thoracic and Cardiovascular Surgeons of Asia\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.5761/atcs.ra.22-00103\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2022/7/15 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of thoracic and cardiovascular surgery : official journal of the Association of Thoracic and Cardiovascular Surgeons of Asia","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.5761/atcs.ra.22-00103","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/7/15 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
Surgical Management for Systolic Anterior Motion (SAM) of the Mitral Valve in Obstructive Hypertrophic Myopathy.
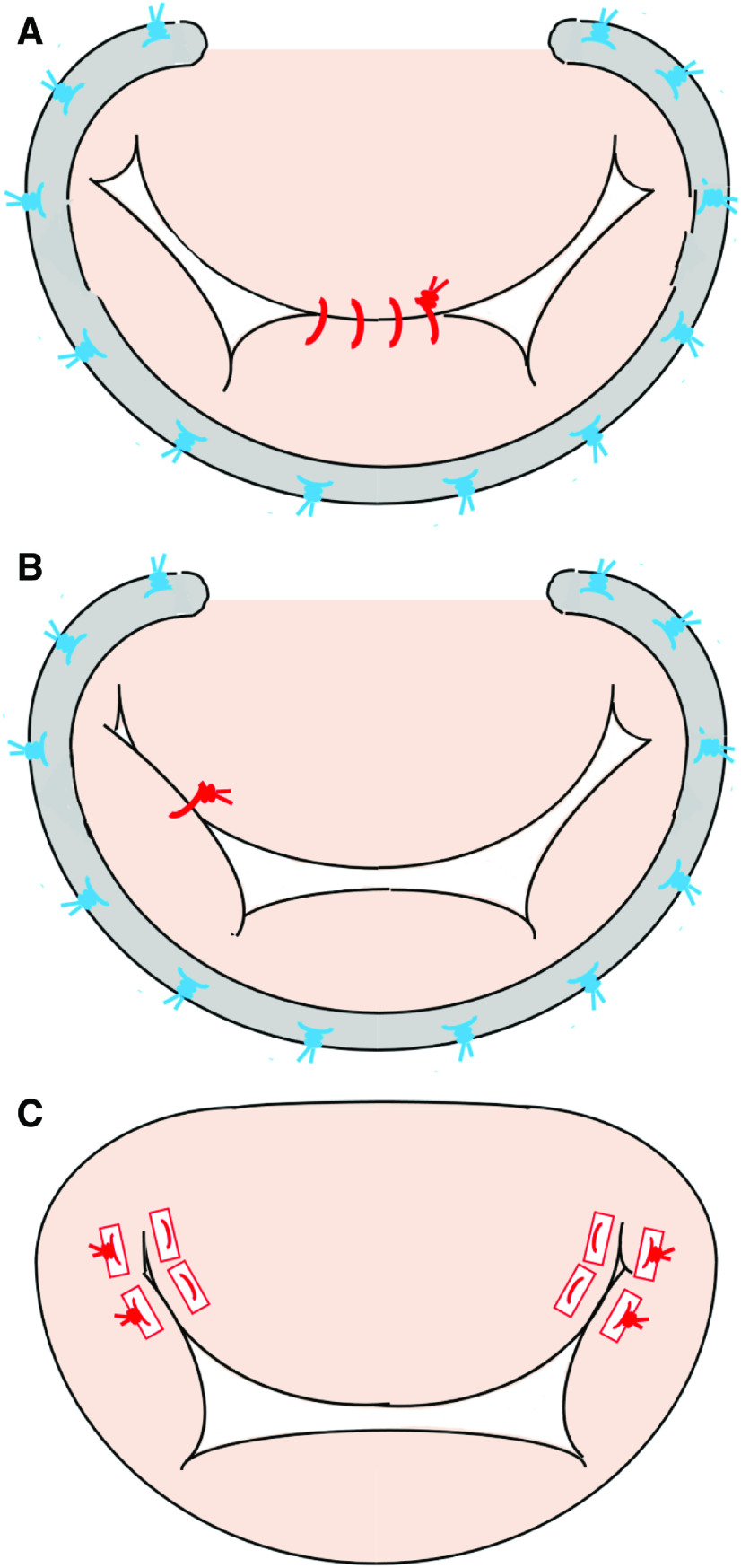
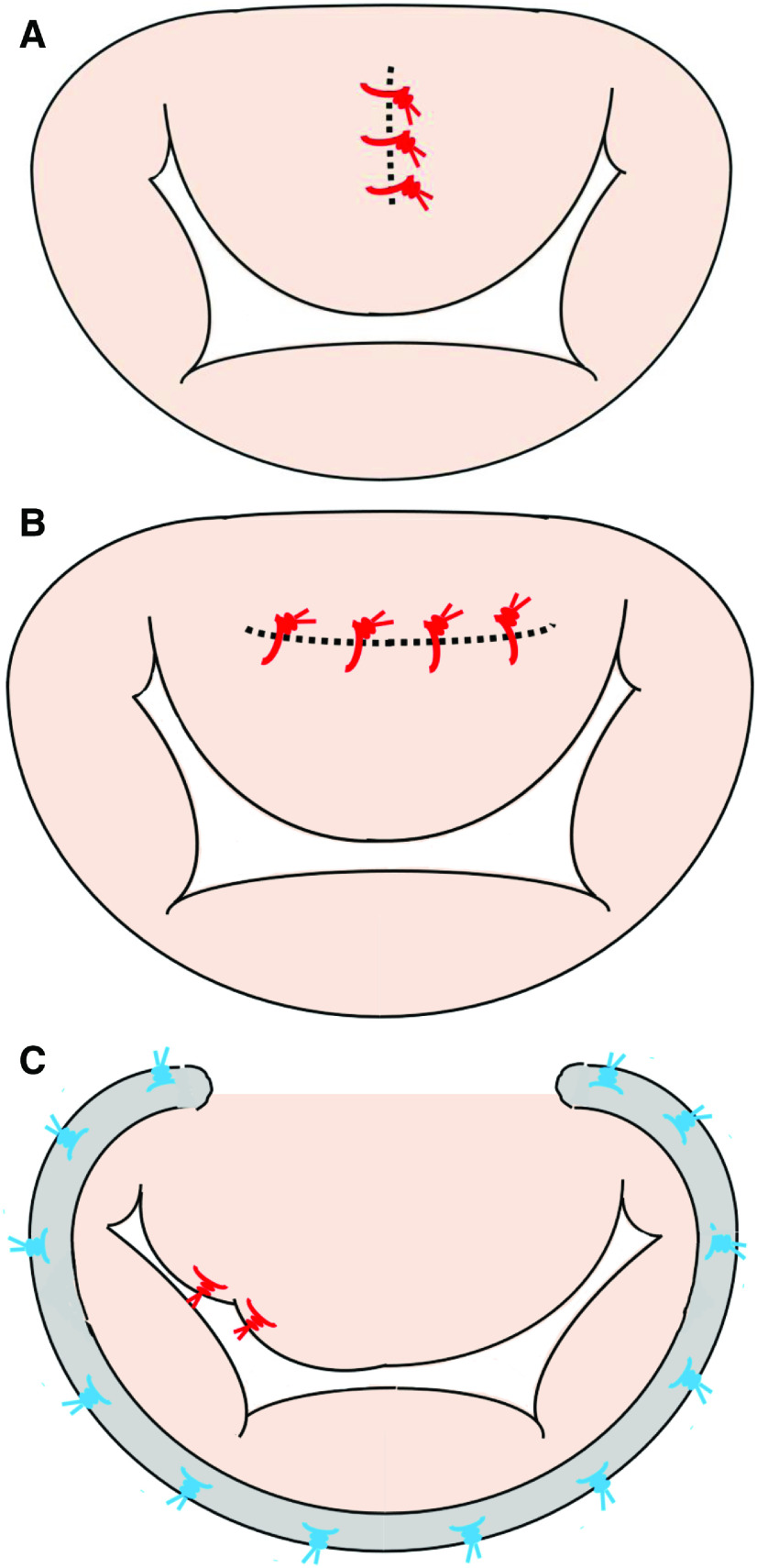
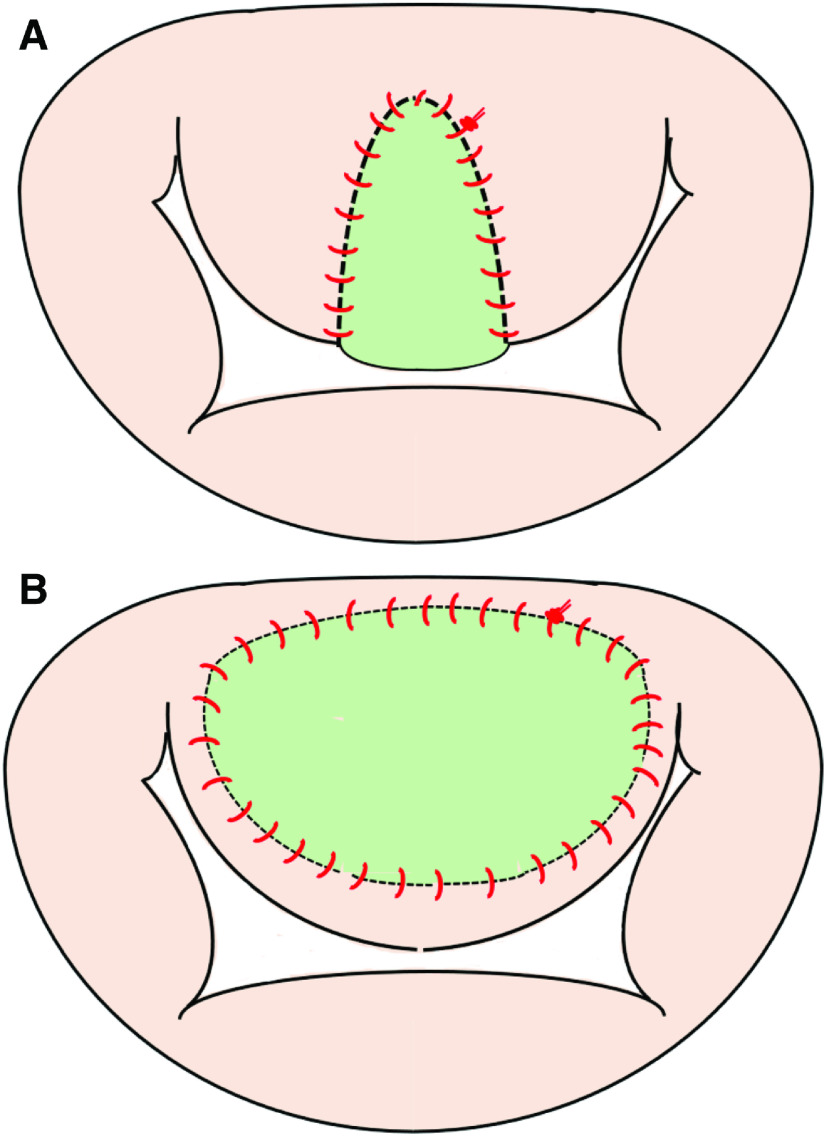
In patients with obstructive hypertrophic cardiomyopathy, left ventricular outflow tract (LVOT) obstruction can be created by the hypertrophic interventricular septum (IVS) as well as systolic anterior motion (SAM) of the anterior mitral leaflet (AML). Sufficient septal myectomy is a fundamental surgical technique to treat LVOT obstruction, however, direct surgical management for SAM is another key aspect. Besides the hypertrophic IVS, mitral valve, subvalvular apparatus, and papillary muscle may play important role for SAM and several surgical techniques have been proposed to treat SAM in literature. In this review, each surgical technique is classified by the anatomical structure on which the surgical procedure is applied. The AML is the main surgical site and is applied with plication (vertical plication, resection-plication-release strategy), extension (the AML extension, transverse incision of the AML), sutured (edge-to-edge repair, anterior leaflet retention plasty), or traction (floating stitch, papillary muscle-to-anterior annulus stitches, paradoxical stitches, transposition of a directed chorda tendinea to the AML). Height reduction of the posterior mitral valve leaflet and papillary muscle reorientation are other techniques. We should understand theoretical aspects of each technique on correction of anatomical and functional abnormalities of the structure and should apply them under proper indication.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
