Brian Kerr, Rebabonye B Pharithi, Matthew Barrett, Carmel Halley, Joe Gallagher, Mark Ledwidge, Kenneth McDonald
{"title":"血管紧张素受体奈普利素抑制剂用于HFrEF:这是第一个导致利尿需求大幅减少的疾病修饰治疗药物类别吗?","authors":"Brian Kerr, Rebabonye B Pharithi, Matthew Barrett, Carmel Halley, Joe Gallagher, Mark Ledwidge, Kenneth McDonald","doi":"10.36628/ijhf.2020.0043","DOIUrl":null,"url":null,"abstract":"<p><p>Despite significant advances in disease modifying therapy in heart failure (HF), diuretics have remained the cornerstone of volume management in all HF phenotypes. Diuretics, alongside their definite acute haemodynamic and symptomatic benefits, also possess many possible deleterious side effects. Moreover, questions remain regarding the prognostic impact of chronic diuretic use. To date, few data exist pertaining to diuretic reduction as a result of individual traditional guideline directed medical therapy in HF with reduced ejection fraction (HFrEF). However, diuretic reduction has been demonstrated with sacubitril/valsartan (angiotensin receptor-neprilysin inhibitor [ARNi]) from the PARADIGM study, as well as, post-marketing reports from our own group and others. Whether the ARNi compound represents the dawn of a new era, where effective therapies will have a more noticeable reduction on diuretic need, remains to be seen. The emergence of sodium glucose transport 2 inhibitors and guanylate cyclase stimulators may further exemplify this issue and potentially extend this benefit to HF patients outside of the HFrEF phenotype. In conclusion, emerging new therapies in HFrEF could reduce the reliance on diuretics in the management of this phenotype of HF. These developments further highlight the clinical importance to continually assess an individual's diuretic requirements through careful volume assessment.</p>","PeriodicalId":14058,"journal":{"name":"International Journal of Heart Failure","volume":"3 2","pages":"106-116"},"PeriodicalIF":0.0000,"publicationDate":"2021-02-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/73/a7/ijhf-3-106.PMC9536695.pdf","citationCount":"2","resultStr":"{\"title\":\"Angiotensin Receptor Neprilysin Inhibitors in HFrEF: Is This the First Disease Modifying Therapy Drug Class Leading to a Substantial Reduction in Diuretic Need?\",\"authors\":\"Brian Kerr, Rebabonye B Pharithi, Matthew Barrett, Carmel Halley, Joe Gallagher, Mark Ledwidge, Kenneth McDonald\",\"doi\":\"10.36628/ijhf.2020.0043\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Despite significant advances in disease modifying therapy in heart failure (HF), diuretics have remained the cornerstone of volume management in all HF phenotypes. Diuretics, alongside their definite acute haemodynamic and symptomatic benefits, also possess many possible deleterious side effects. Moreover, questions remain regarding the prognostic impact of chronic diuretic use. To date, few data exist pertaining to diuretic reduction as a result of individual traditional guideline directed medical therapy in HF with reduced ejection fraction (HFrEF). However, diuretic reduction has been demonstrated with sacubitril/valsartan (angiotensin receptor-neprilysin inhibitor [ARNi]) from the PARADIGM study, as well as, post-marketing reports from our own group and others. Whether the ARNi compound represents the dawn of a new era, where effective therapies will have a more noticeable reduction on diuretic need, remains to be seen. The emergence of sodium glucose transport 2 inhibitors and guanylate cyclase stimulators may further exemplify this issue and potentially extend this benefit to HF patients outside of the HFrEF phenotype. In conclusion, emerging new therapies in HFrEF could reduce the reliance on diuretics in the management of this phenotype of HF. These developments further highlight the clinical importance to continually assess an individual's diuretic requirements through careful volume assessment.</p>\",\"PeriodicalId\":14058,\"journal\":{\"name\":\"International Journal of Heart Failure\",\"volume\":\"3 2\",\"pages\":\"106-116\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2021-02-25\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/73/a7/ijhf-3-106.PMC9536695.pdf\",\"citationCount\":\"2\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"International Journal of Heart Failure\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.36628/ijhf.2020.0043\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2021/4/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Journal of Heart Failure","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.36628/ijhf.2020.0043","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/4/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Angiotensin Receptor Neprilysin Inhibitors in HFrEF: Is This the First Disease Modifying Therapy Drug Class Leading to a Substantial Reduction in Diuretic Need?
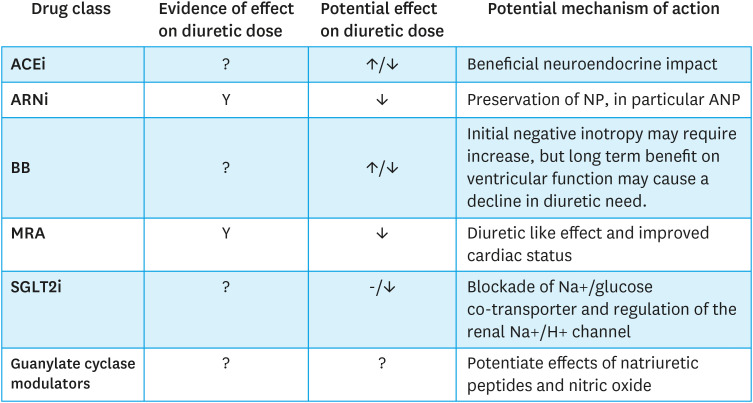
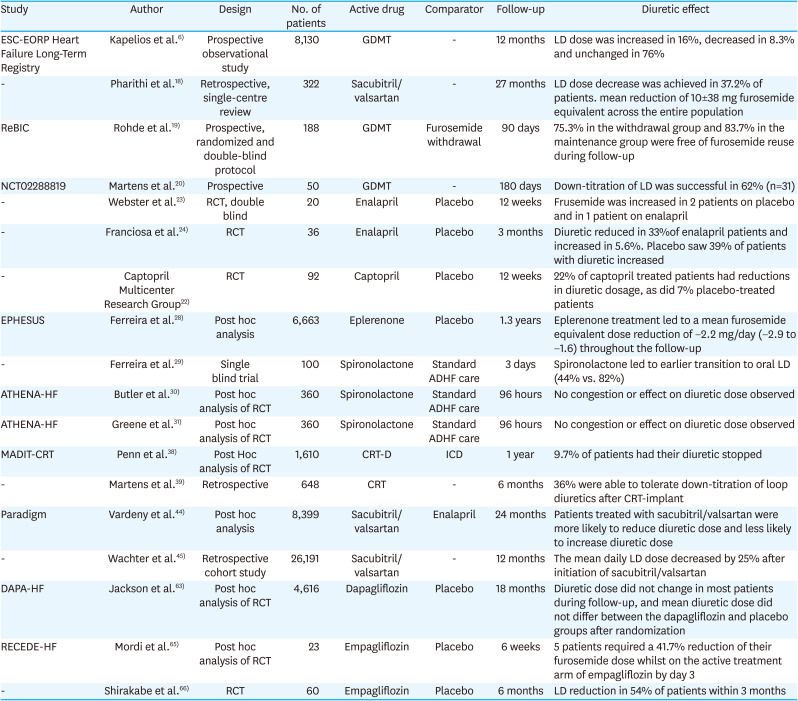
Despite significant advances in disease modifying therapy in heart failure (HF), diuretics have remained the cornerstone of volume management in all HF phenotypes. Diuretics, alongside their definite acute haemodynamic and symptomatic benefits, also possess many possible deleterious side effects. Moreover, questions remain regarding the prognostic impact of chronic diuretic use. To date, few data exist pertaining to diuretic reduction as a result of individual traditional guideline directed medical therapy in HF with reduced ejection fraction (HFrEF). However, diuretic reduction has been demonstrated with sacubitril/valsartan (angiotensin receptor-neprilysin inhibitor [ARNi]) from the PARADIGM study, as well as, post-marketing reports from our own group and others. Whether the ARNi compound represents the dawn of a new era, where effective therapies will have a more noticeable reduction on diuretic need, remains to be seen. The emergence of sodium glucose transport 2 inhibitors and guanylate cyclase stimulators may further exemplify this issue and potentially extend this benefit to HF patients outside of the HFrEF phenotype. In conclusion, emerging new therapies in HFrEF could reduce the reliance on diuretics in the management of this phenotype of HF. These developments further highlight the clinical importance to continually assess an individual's diuretic requirements through careful volume assessment.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
