{"title":"印度三级医疗中心心力衰竭伴射血分数降低患者出院后60天再住院率及其决定因素","authors":"Kakasaheb H Bhosale, Ranjit Kumar Nath, Neeraj Pandit, Puneet Agarwal, Shripad Khairnar, Balram Yadav, Sulabh Chandrakar","doi":"10.36628/ijhf.2020.0007","DOIUrl":null,"url":null,"abstract":"<p><strong>Background and objectives: </strong>Identifying the patients with acute heart failure (HF) at high risk for rehospitalization after hospital discharge will enable proper optimization of treatment. This study is aimed to evaluate the rehospitalization rate at 60 days of discharge and their predictors in patients of chronic heart failure with reduced ejection fraction (HFrEF).</p><p><strong>Methods: </strong>This prospective observational study enrolled patients with left ventricle ejection fraction (LVEF) <40%, who were admitted because of acute decompensation. Patients were followed for 60 days to analyze rehospitalization rate and its predictors.</p><p><strong>Results: </strong>Of 103 HFrEF patients (74% male; mean age 55.8 years) enrolled, 7 patients died during index admission and 3 patients lost to follow up. The 60-day rehospitalization rate was 37% (34/93). We studied 23 clinical and 9 biochemical predictors of rehospitalization. Out of 34 events of rehospitalization, 79.41% (n=28) was due to cardiac cause followed by respiratory 5.8% (n=2), renal 5.8% (n=2) and others 5.8% (n=2). Among all the parameters, on logistic regression analysis having longer length of index hospital stay (>7 days) (52.8% vs. 28.8%; odds ratio [OR], 1.79; confidence interval [CI], 1.2-7.25; p=0.040) and chronic kidney disease (CKD) (26.5% vs. 8.5%; OR, 3.06; CI, 1.1-57.04; p=0.050) independently increased the risk of rehospitalization at 60 days of discharge. Further higher haemoglobin level (11.3 vs. 9.9 gm/dL; OR, 0.71; CI, 0.48-0.97; p=0.050) and higher LVEF at index admission (30.4% vs. 26.5%; OR, 0.87; CI, 0.75-0.99; p=0.049) were associated with decreased the risk of rehospitalization.</p><p><strong>Conclusions: </strong>Our study reveals that patients with HFrEF have significantly higher rehospitalization rate (37%) and in-hospital mortality rates (6.78%) of any chronic cardiac disease conditions. Correction of low hemoglobin and special care in those who are having very low LVEF, CKD and longer length of stay, including tailored therapy and frequent visits may play an important role in preventing future rehospitalization in these patients.</p>","PeriodicalId":14058,"journal":{"name":"International Journal of Heart Failure","volume":"2 2","pages":"131-144"},"PeriodicalIF":0.0000,"publicationDate":"2020-04-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/66/b2/ijhf-2-131.PMC9536659.pdf","citationCount":"8","resultStr":"{\"title\":\"Rate of Rehospitalization in 60 Days of Discharge and It's Determinants in Patients with Heart Failure with Reduced Ejection Fraction in a Tertiary Care Centre in India.\",\"authors\":\"Kakasaheb H Bhosale, Ranjit Kumar Nath, Neeraj Pandit, Puneet Agarwal, Shripad Khairnar, Balram Yadav, Sulabh Chandrakar\",\"doi\":\"10.36628/ijhf.2020.0007\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background and objectives: </strong>Identifying the patients with acute heart failure (HF) at high risk for rehospitalization after hospital discharge will enable proper optimization of treatment. This study is aimed to evaluate the rehospitalization rate at 60 days of discharge and their predictors in patients of chronic heart failure with reduced ejection fraction (HFrEF).</p><p><strong>Methods: </strong>This prospective observational study enrolled patients with left ventricle ejection fraction (LVEF) <40%, who were admitted because of acute decompensation. Patients were followed for 60 days to analyze rehospitalization rate and its predictors.</p><p><strong>Results: </strong>Of 103 HFrEF patients (74% male; mean age 55.8 years) enrolled, 7 patients died during index admission and 3 patients lost to follow up. The 60-day rehospitalization rate was 37% (34/93). We studied 23 clinical and 9 biochemical predictors of rehospitalization. Out of 34 events of rehospitalization, 79.41% (n=28) was due to cardiac cause followed by respiratory 5.8% (n=2), renal 5.8% (n=2) and others 5.8% (n=2). Among all the parameters, on logistic regression analysis having longer length of index hospital stay (>7 days) (52.8% vs. 28.8%; odds ratio [OR], 1.79; confidence interval [CI], 1.2-7.25; p=0.040) and chronic kidney disease (CKD) (26.5% vs. 8.5%; OR, 3.06; CI, 1.1-57.04; p=0.050) independently increased the risk of rehospitalization at 60 days of discharge. Further higher haemoglobin level (11.3 vs. 9.9 gm/dL; OR, 0.71; CI, 0.48-0.97; p=0.050) and higher LVEF at index admission (30.4% vs. 26.5%; OR, 0.87; CI, 0.75-0.99; p=0.049) were associated with decreased the risk of rehospitalization.</p><p><strong>Conclusions: </strong>Our study reveals that patients with HFrEF have significantly higher rehospitalization rate (37%) and in-hospital mortality rates (6.78%) of any chronic cardiac disease conditions. Correction of low hemoglobin and special care in those who are having very low LVEF, CKD and longer length of stay, including tailored therapy and frequent visits may play an important role in preventing future rehospitalization in these patients.</p>\",\"PeriodicalId\":14058,\"journal\":{\"name\":\"International Journal of Heart Failure\",\"volume\":\"2 2\",\"pages\":\"131-144\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2020-04-21\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/66/b2/ijhf-2-131.PMC9536659.pdf\",\"citationCount\":\"8\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"International Journal of Heart Failure\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.36628/ijhf.2020.0007\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2020/4/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Journal of Heart Failure","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.36628/ijhf.2020.0007","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2020/4/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 8
摘要
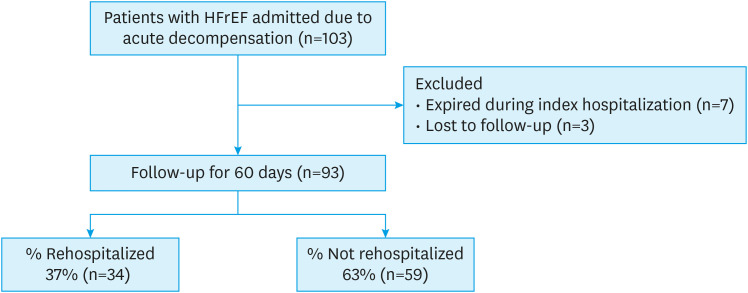
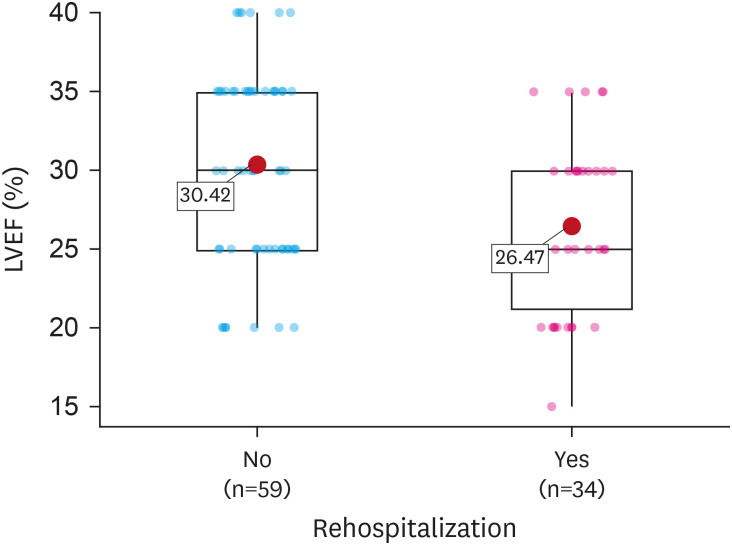
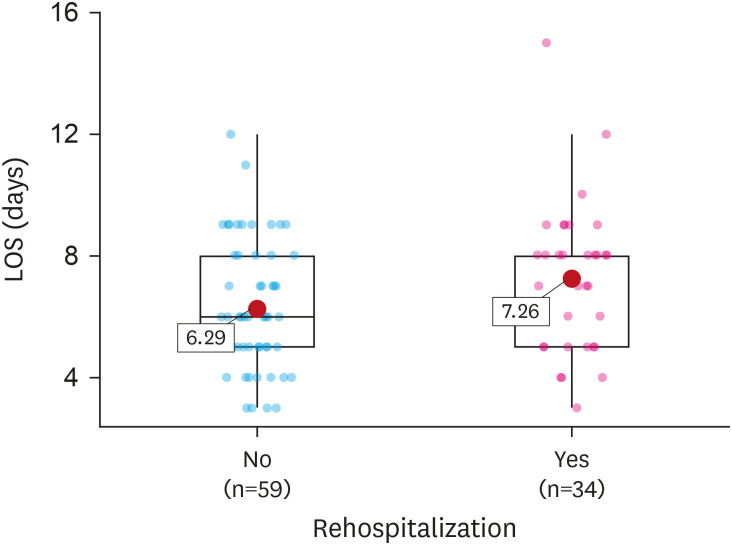
背景与目的:识别出院后再次住院的高危急性心力衰竭(HF)患者将有助于适当优化治疗。本研究旨在评估慢性心力衰竭伴射血分数降低(HFrEF)患者出院后60天的再住院率及其预测因素。方法:本前瞻性观察研究纳入了左心室射血分数(LVEF)患者。结果:103例HFrEF患者(74%男性;平均年龄55.8岁,入院时死亡7例,失访3例。60天再住院率为37%(34/93)。我们研究了23项临床和9项再住院的生化预测指标。34例再住院事件中,心脏原因占79.41% (n=28),其次是呼吸原因5.8% (n=2),肾脏原因5.8% (n=2),其他原因5.8% (n=2)。在所有参数中,经logistic回归分析,指标住院时间较长的患者(>7天)(52.8% vs. 28.8%;优势比[OR], 1.79;置信区间[CI], 1.2-7.25;p=0.040)和慢性肾脏疾病(CKD) (26.5% vs. 8.5%;或者,3.06;CI, 1.1 - -57.04;P =0.050)独立增加出院后60天再住院的风险。血红蛋白进一步升高(11.3 vs. 9.9 gm/dL;或者,0.71;CI, 0.48 - -0.97;p=0.050),且指数进场时LVEF较高(30.4% vs. 26.5%;或者,0.87;CI, 0.75 - -0.99;P =0.049)与再住院风险降低相关。结论:我们的研究表明,HFrEF患者的再住院率(37%)和住院死亡率(6.78%)明显高于任何慢性心脏病。对于LVEF非常低、CKD和住院时间较长的患者,纠正低血红蛋白和特殊护理,包括量身定制的治疗和频繁的就诊,可能在预防这些患者未来再次住院方面发挥重要作用。
Rate of Rehospitalization in 60 Days of Discharge and It's Determinants in Patients with Heart Failure with Reduced Ejection Fraction in a Tertiary Care Centre in India.
Background and objectives: Identifying the patients with acute heart failure (HF) at high risk for rehospitalization after hospital discharge will enable proper optimization of treatment. This study is aimed to evaluate the rehospitalization rate at 60 days of discharge and their predictors in patients of chronic heart failure with reduced ejection fraction (HFrEF).
Methods: This prospective observational study enrolled patients with left ventricle ejection fraction (LVEF) <40%, who were admitted because of acute decompensation. Patients were followed for 60 days to analyze rehospitalization rate and its predictors.
Results: Of 103 HFrEF patients (74% male; mean age 55.8 years) enrolled, 7 patients died during index admission and 3 patients lost to follow up. The 60-day rehospitalization rate was 37% (34/93). We studied 23 clinical and 9 biochemical predictors of rehospitalization. Out of 34 events of rehospitalization, 79.41% (n=28) was due to cardiac cause followed by respiratory 5.8% (n=2), renal 5.8% (n=2) and others 5.8% (n=2). Among all the parameters, on logistic regression analysis having longer length of index hospital stay (>7 days) (52.8% vs. 28.8%; odds ratio [OR], 1.79; confidence interval [CI], 1.2-7.25; p=0.040) and chronic kidney disease (CKD) (26.5% vs. 8.5%; OR, 3.06; CI, 1.1-57.04; p=0.050) independently increased the risk of rehospitalization at 60 days of discharge. Further higher haemoglobin level (11.3 vs. 9.9 gm/dL; OR, 0.71; CI, 0.48-0.97; p=0.050) and higher LVEF at index admission (30.4% vs. 26.5%; OR, 0.87; CI, 0.75-0.99; p=0.049) were associated with decreased the risk of rehospitalization.
Conclusions: Our study reveals that patients with HFrEF have significantly higher rehospitalization rate (37%) and in-hospital mortality rates (6.78%) of any chronic cardiac disease conditions. Correction of low hemoglobin and special care in those who are having very low LVEF, CKD and longer length of stay, including tailored therapy and frequent visits may play an important role in preventing future rehospitalization in these patients.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
