Wardah Rafaqat, Mohammad Hamza Bajwa, Meher Angez, Syed Ather Enam
{"title":"成人颅咽管瘤经鼻内窥镜与经颅切除术的手术效果:荟萃分析。","authors":"Wardah Rafaqat, Mohammad Hamza Bajwa, Meher Angez, Syed Ather Enam","doi":"10.14791/btrt.2022.0014","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The endoscopic endonasal approach (EEA) has been gaining popularity for resection of adult craniopharyngiomas. However, the safety and effectiveness of the procedure in comparison to the traditional transcranial approach (TCA) remains unestablished as previous reviews are outdated.</p><p><strong>Methods: </strong>A literature search without language restriction was conducted in PubMed, Cochrane database, and Web of Science from conception to July 9, 2021. Cohort studies and case series that compared EEA with TCA and assessed postoperative complications, recurrence, and 30-day mortality were included. Articles, where data for adult populations could not be extracted or calculated, were excluded. Article selection and data extraction in a predesigned data extraction form were conducted in duplicate. Pooled participant data were included in a random-effects model.</p><p><strong>Results: </strong>The search yielded 227 articles, from which eight cohort studies containing 11,395 patients were included (EEA: 6,614 patients, TCA: 4,781 patients). Six studies were good quality and two were fair quality according to the Newcastle Ottawa Scale. There were significantly higher rates of cerebrospinal fluid leak (risk ratio [RR]=0.23, 95% confidence interval [CI] 0.17-0.32, <i>p</i><0.00001, I²=0%) and lower rates of postoperative hypopituitarism (RR=1.40, 95% CI 1.30-1.51, <i>p</i><0.00001, I²=0%), hydrocephalus (RR=6.95, 95% CI 5.78-8.36, <i>p</i><0.00001, I²=0%), visual impairment (RR=1.52, 95% CI 1.34-1.73, <i>p</i><0.00001, I²=0%), and 30-day mortality (RR=5.63, 95% CI 3.87-8.19, <i>p</i><0.00001, I²=0%) after EEA. Non-significant lower rates of postoperative diabetes insipidus (RR=1.12, 95% CI 0.78-1.61, <i>p</i>=0.53, I²=85%) and recurrence of tumor (RR=2.69, 95% CI 0.35-20.81, <i>p</i>=0.34, I²=47%) were seen after EEA.</p><p><strong>Conclusion: </strong>EEA may be associated with reduced postoperative hypopituitarism, hydrocephalus, visual impairment, and 30-day mortality and higher rates of cerebrospinal fluid leak. These findings do not account for differences in tumor size and extension between the EEA and TCA cohorts. Further research on patients with comparable tumor characteristics is required to fully assess outcomes.</p>","PeriodicalId":72453,"journal":{"name":"Brain tumor research and treatment","volume":"10 4","pages":"226-236"},"PeriodicalIF":0.0000,"publicationDate":"2022-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/a8/45/btrt-10-226.PMC9650119.pdf","citationCount":"2","resultStr":"{\"title\":\"Surgical Outcomes of Endoscopic Endonasal Versus Transcranial Resections of Adult Craniopharyngioma: A Meta-Analysis.\",\"authors\":\"Wardah Rafaqat, Mohammad Hamza Bajwa, Meher Angez, Syed Ather Enam\",\"doi\":\"10.14791/btrt.2022.0014\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>The endoscopic endonasal approach (EEA) has been gaining popularity for resection of adult craniopharyngiomas. However, the safety and effectiveness of the procedure in comparison to the traditional transcranial approach (TCA) remains unestablished as previous reviews are outdated.</p><p><strong>Methods: </strong>A literature search without language restriction was conducted in PubMed, Cochrane database, and Web of Science from conception to July 9, 2021. Cohort studies and case series that compared EEA with TCA and assessed postoperative complications, recurrence, and 30-day mortality were included. Articles, where data for adult populations could not be extracted or calculated, were excluded. Article selection and data extraction in a predesigned data extraction form were conducted in duplicate. Pooled participant data were included in a random-effects model.</p><p><strong>Results: </strong>The search yielded 227 articles, from which eight cohort studies containing 11,395 patients were included (EEA: 6,614 patients, TCA: 4,781 patients). Six studies were good quality and two were fair quality according to the Newcastle Ottawa Scale. There were significantly higher rates of cerebrospinal fluid leak (risk ratio [RR]=0.23, 95% confidence interval [CI] 0.17-0.32, <i>p</i><0.00001, I²=0%) and lower rates of postoperative hypopituitarism (RR=1.40, 95% CI 1.30-1.51, <i>p</i><0.00001, I²=0%), hydrocephalus (RR=6.95, 95% CI 5.78-8.36, <i>p</i><0.00001, I²=0%), visual impairment (RR=1.52, 95% CI 1.34-1.73, <i>p</i><0.00001, I²=0%), and 30-day mortality (RR=5.63, 95% CI 3.87-8.19, <i>p</i><0.00001, I²=0%) after EEA. Non-significant lower rates of postoperative diabetes insipidus (RR=1.12, 95% CI 0.78-1.61, <i>p</i>=0.53, I²=85%) and recurrence of tumor (RR=2.69, 95% CI 0.35-20.81, <i>p</i>=0.34, I²=47%) were seen after EEA.</p><p><strong>Conclusion: </strong>EEA may be associated with reduced postoperative hypopituitarism, hydrocephalus, visual impairment, and 30-day mortality and higher rates of cerebrospinal fluid leak. These findings do not account for differences in tumor size and extension between the EEA and TCA cohorts. Further research on patients with comparable tumor characteristics is required to fully assess outcomes.</p>\",\"PeriodicalId\":72453,\"journal\":{\"name\":\"Brain tumor research and treatment\",\"volume\":\"10 4\",\"pages\":\"226-236\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2022-10-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/a8/45/btrt-10-226.PMC9650119.pdf\",\"citationCount\":\"2\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Brain tumor research and treatment\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.14791/btrt.2022.0014\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Brain tumor research and treatment","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14791/btrt.2022.0014","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 2
摘要
背景:鼻内窥镜入路(EEA)在成人颅咽管瘤切除术中越来越受欢迎。然而,与传统的经颅入路(TCA)相比,该手术的安全性和有效性仍未确定,因为以前的综述已经过时。方法:检索PubMed、Cochrane数据库和Web of Science自受孕至2021年7月9日的无语言限制的文献。比较EEA和TCA的队列研究和病例系列,评估术后并发症、复发和30天死亡率。不能提取或计算成人人口数据的文章被排除在外。在预先设计的数据提取表格中进行文章选择和数据提取,一式两份。合并的参与者数据包括在随机效应模型中。结果:检索得到227篇文章,其中8项队列研究纳入11,395例患者(EEA: 6,614例患者,TCA: 4,781例患者)。根据纽卡斯尔渥太华量表,6项研究质量良好,2项质量一般。EEA术后脑脊液漏发生率(危险比[RR]=0.23, 95%可信区间[CI] 0.17-0.32, pppppp=0.53, I²=85%)和肿瘤复发率(RR=2.69, 95% CI 0.35-20.81, p=0.34, I²=47%)显著增高。结论:EEA可能与术后垂体功能减退、脑积水、视力障碍、30天死亡率和脑脊液漏率升高有关。这些发现并不能解释EEA组和TCA组在肿瘤大小和扩展方面的差异。需要对具有相似肿瘤特征的患者进行进一步研究,以充分评估结果。
Surgical Outcomes of Endoscopic Endonasal Versus Transcranial Resections of Adult Craniopharyngioma: A Meta-Analysis.
Background: The endoscopic endonasal approach (EEA) has been gaining popularity for resection of adult craniopharyngiomas. However, the safety and effectiveness of the procedure in comparison to the traditional transcranial approach (TCA) remains unestablished as previous reviews are outdated.
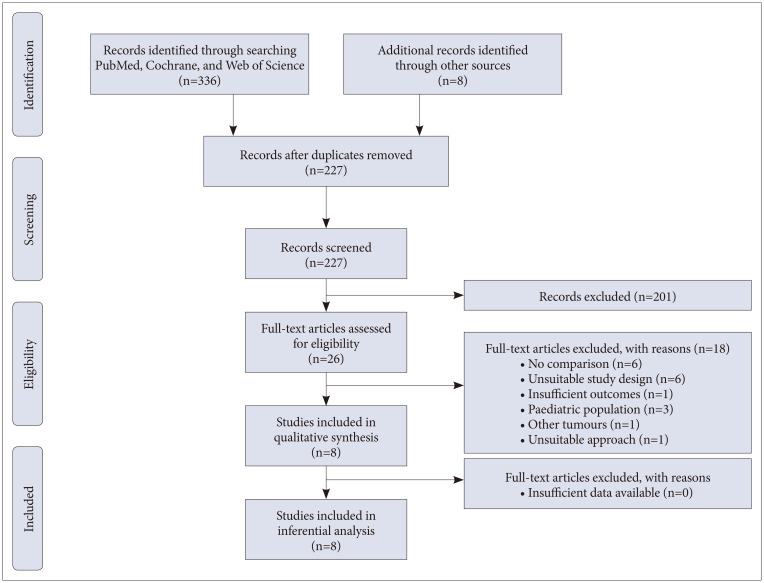
Methods: A literature search without language restriction was conducted in PubMed, Cochrane database, and Web of Science from conception to July 9, 2021. Cohort studies and case series that compared EEA with TCA and assessed postoperative complications, recurrence, and 30-day mortality were included. Articles, where data for adult populations could not be extracted or calculated, were excluded. Article selection and data extraction in a predesigned data extraction form were conducted in duplicate. Pooled participant data were included in a random-effects model.
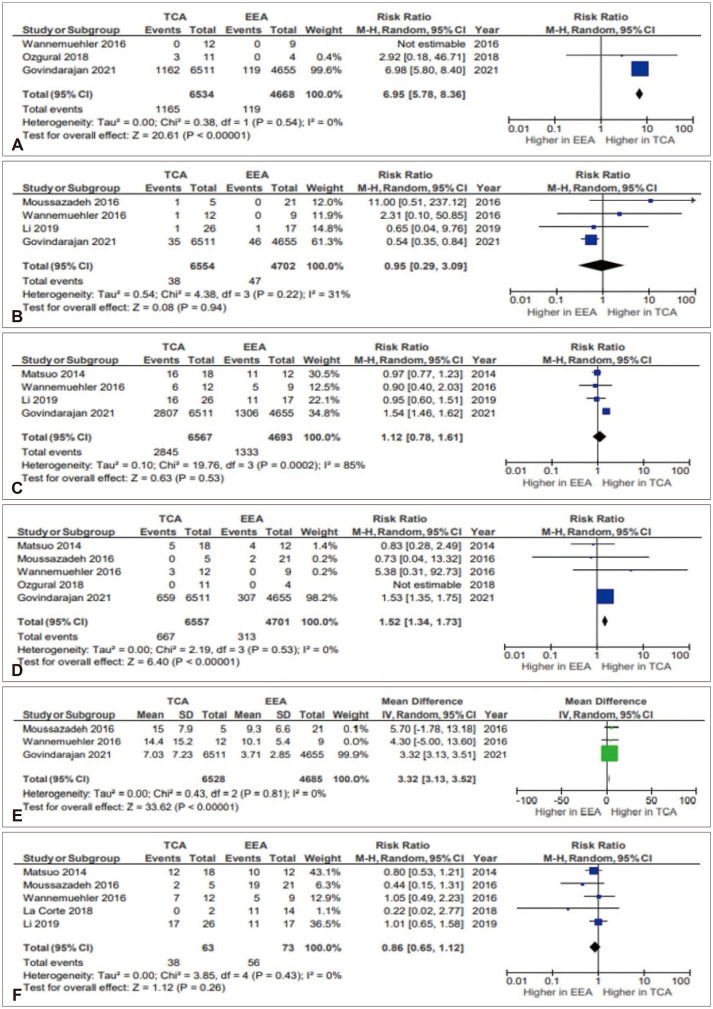
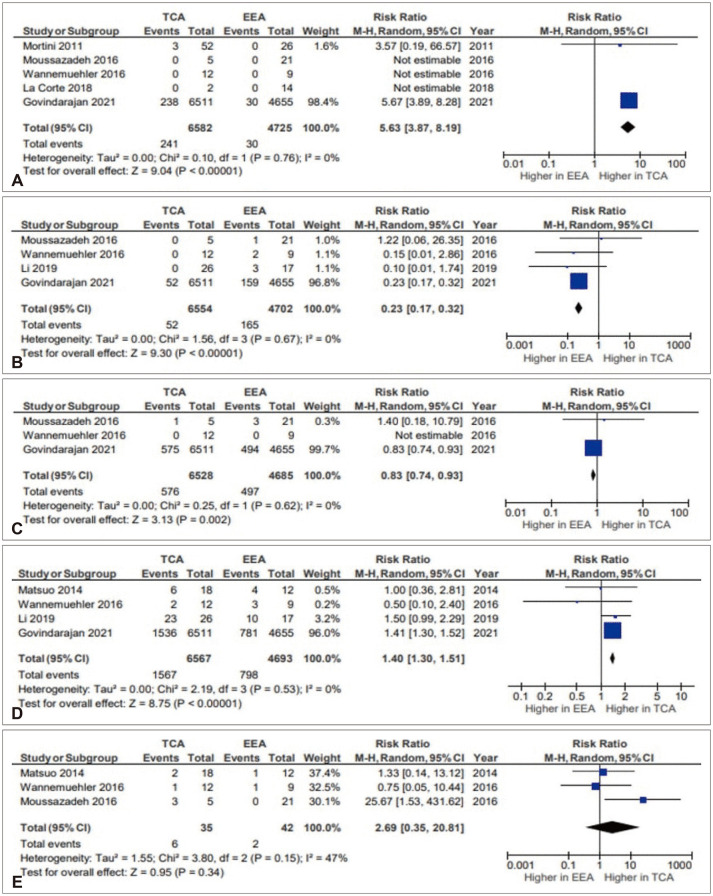
Results: The search yielded 227 articles, from which eight cohort studies containing 11,395 patients were included (EEA: 6,614 patients, TCA: 4,781 patients). Six studies were good quality and two were fair quality according to the Newcastle Ottawa Scale. There were significantly higher rates of cerebrospinal fluid leak (risk ratio [RR]=0.23, 95% confidence interval [CI] 0.17-0.32, p<0.00001, I²=0%) and lower rates of postoperative hypopituitarism (RR=1.40, 95% CI 1.30-1.51, p<0.00001, I²=0%), hydrocephalus (RR=6.95, 95% CI 5.78-8.36, p<0.00001, I²=0%), visual impairment (RR=1.52, 95% CI 1.34-1.73, p<0.00001, I²=0%), and 30-day mortality (RR=5.63, 95% CI 3.87-8.19, p<0.00001, I²=0%) after EEA. Non-significant lower rates of postoperative diabetes insipidus (RR=1.12, 95% CI 0.78-1.61, p=0.53, I²=85%) and recurrence of tumor (RR=2.69, 95% CI 0.35-20.81, p=0.34, I²=47%) were seen after EEA.
Conclusion: EEA may be associated with reduced postoperative hypopituitarism, hydrocephalus, visual impairment, and 30-day mortality and higher rates of cerebrospinal fluid leak. These findings do not account for differences in tumor size and extension between the EEA and TCA cohorts. Further research on patients with comparable tumor characteristics is required to fully assess outcomes.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
