Rafael Golpe, Nagore Blanco-Cid, David Dacal-Rivas, Irene Martín-Robles, Iria Veiga, Indhira Guzmán-Peralta, Olalla Castro-Añón, Luis A Pérez-de-Llano
{"title":"生物质烟雾或烟草引起的慢性阻塞性肺疾病严重恶化的发生率和概况","authors":"Rafael Golpe, Nagore Blanco-Cid, David Dacal-Rivas, Irene Martín-Robles, Iria Veiga, Indhira Guzmán-Peralta, Olalla Castro-Añón, Luis A Pérez-de-Llano","doi":"10.4103/atm.atm_155_22","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction and objectives: </strong>Stable chronic obstructive pulmonary disease (COPD) caused by biomass smoke (B-COPD) has some differences from tobacco-induced-COPD (T-COPD), but acute exacerbations (AECOPD) have not been well characterized in B-COPD.</p><p><strong>Objective: </strong>To compare the incidence, characteristics and outcomes of AECOPD in B-COPD with those of T-COPD.</p><p><strong>Methods: </strong>A retrospective observational study that included consecutive patients seen at a specialized COPD clinic (2008-2021). The incidence of severe AECOPD that required hospital admission was studied. For the first AECOPD, the following variables were recorded: fever, coexistence of pneumonia, purulent sputum, eosinophil count, neutrophil to lymphocyte ratio, hypercapnia, and respiratory acidosis. Outcome variables were intensive care unit (ICU) admission, length of hospital stay, and mortality within 1 month of hospital admission.</p><p><strong>Results: </strong>Of 1060 subjects, 195 (18.4%) belonged to the B-COPD group and 865 (81.6%) to the T-COPD group. During a follow-up of 67.9 (37.8-98.8) months, 75 (38.4%) patients in the B-COPD group and 319 (36.8%) in the T-COPD group suffered at least one severe AECOPD. The only difference between groups was in a higher risk of ICU admission for the T-COPD group. The incidence, characteristics, and the rest of the outcomes of AECOPD were similar for both groups.</p><p><strong>Conclusion: </strong>AECOPD are similar events for B-COPD and T-COPD and should be managed similarly.</p>","PeriodicalId":50760,"journal":{"name":"Annals of Thoracic Medicine","volume":"17 4","pages":"193-198"},"PeriodicalIF":2.3000,"publicationDate":"2022-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/f0/6d/ATM-17-193.PMC9662078.pdf","citationCount":"0","resultStr":"{\"title\":\"Incidence and profile of severe exacerbations of chronic obstructive pulmonary disease due to biomass smoke or tobacco.\",\"authors\":\"Rafael Golpe, Nagore Blanco-Cid, David Dacal-Rivas, Irene Martín-Robles, Iria Veiga, Indhira Guzmán-Peralta, Olalla Castro-Añón, Luis A Pérez-de-Llano\",\"doi\":\"10.4103/atm.atm_155_22\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction and objectives: </strong>Stable chronic obstructive pulmonary disease (COPD) caused by biomass smoke (B-COPD) has some differences from tobacco-induced-COPD (T-COPD), but acute exacerbations (AECOPD) have not been well characterized in B-COPD.</p><p><strong>Objective: </strong>To compare the incidence, characteristics and outcomes of AECOPD in B-COPD with those of T-COPD.</p><p><strong>Methods: </strong>A retrospective observational study that included consecutive patients seen at a specialized COPD clinic (2008-2021). The incidence of severe AECOPD that required hospital admission was studied. For the first AECOPD, the following variables were recorded: fever, coexistence of pneumonia, purulent sputum, eosinophil count, neutrophil to lymphocyte ratio, hypercapnia, and respiratory acidosis. Outcome variables were intensive care unit (ICU) admission, length of hospital stay, and mortality within 1 month of hospital admission.</p><p><strong>Results: </strong>Of 1060 subjects, 195 (18.4%) belonged to the B-COPD group and 865 (81.6%) to the T-COPD group. During a follow-up of 67.9 (37.8-98.8) months, 75 (38.4%) patients in the B-COPD group and 319 (36.8%) in the T-COPD group suffered at least one severe AECOPD. The only difference between groups was in a higher risk of ICU admission for the T-COPD group. The incidence, characteristics, and the rest of the outcomes of AECOPD were similar for both groups.</p><p><strong>Conclusion: </strong>AECOPD are similar events for B-COPD and T-COPD and should be managed similarly.</p>\",\"PeriodicalId\":50760,\"journal\":{\"name\":\"Annals of Thoracic Medicine\",\"volume\":\"17 4\",\"pages\":\"193-198\"},\"PeriodicalIF\":2.3000,\"publicationDate\":\"2022-10-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/f0/6d/ATM-17-193.PMC9662078.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Annals of Thoracic Medicine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.4103/atm.atm_155_22\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2022/10/7 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of Thoracic Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.4103/atm.atm_155_22","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/10/7 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Incidence and profile of severe exacerbations of chronic obstructive pulmonary disease due to biomass smoke or tobacco.
Introduction and objectives: Stable chronic obstructive pulmonary disease (COPD) caused by biomass smoke (B-COPD) has some differences from tobacco-induced-COPD (T-COPD), but acute exacerbations (AECOPD) have not been well characterized in B-COPD.
Objective: To compare the incidence, characteristics and outcomes of AECOPD in B-COPD with those of T-COPD.
Methods: A retrospective observational study that included consecutive patients seen at a specialized COPD clinic (2008-2021). The incidence of severe AECOPD that required hospital admission was studied. For the first AECOPD, the following variables were recorded: fever, coexistence of pneumonia, purulent sputum, eosinophil count, neutrophil to lymphocyte ratio, hypercapnia, and respiratory acidosis. Outcome variables were intensive care unit (ICU) admission, length of hospital stay, and mortality within 1 month of hospital admission.
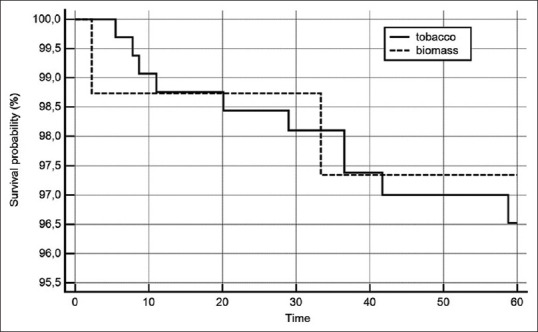
Results: Of 1060 subjects, 195 (18.4%) belonged to the B-COPD group and 865 (81.6%) to the T-COPD group. During a follow-up of 67.9 (37.8-98.8) months, 75 (38.4%) patients in the B-COPD group and 319 (36.8%) in the T-COPD group suffered at least one severe AECOPD. The only difference between groups was in a higher risk of ICU admission for the T-COPD group. The incidence, characteristics, and the rest of the outcomes of AECOPD were similar for both groups.
Conclusion: AECOPD are similar events for B-COPD and T-COPD and should be managed similarly.
期刊介绍:
The journal will cover studies related to multidisciplinary specialties of chest medicine, such as adult and pediatrics pulmonology, thoracic surgery, critical care medicine, respiratory care, transplantation, sleep medicine, related basic medical sciences, and more. The journal also features basic science, special reports, case reports, board review , and more. Editorials and communications to the editor that explore controversial issues and encourage further discussion by physicians dealing with chest medicine.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
