Ali Ibrahim, Nour Moukalled, Rami Mahfouz, Jean El Cheikh, Ali Bazarbachi, Iman Abou Dalle
{"title":"尼洛替尼选择性切换到伊马替尼治疗新诊断的慢性期慢性髓性白血病的安全性和有效性。","authors":"Ali Ibrahim, Nour Moukalled, Rami Mahfouz, Jean El Cheikh, Ali Bazarbachi, Iman Abou Dalle","doi":"10.1007/s44228-022-00001-x","DOIUrl":null,"url":null,"abstract":"<p><p>The treatment of newly diagnosed chronic phase chronic myeloid leukemia (CML) with nilotinib has resulted in a higher rate of major molecular (MMR) and complete cytogenetic response (CCyR) at 12 months compared to imatinib but at a higher cumulative cost and increased risk of serious adverse events. To maintain long-term efficacy and minimize both toxicity and costs, we aimed at evaluating in a prospective single-center trial the efficacy and safety of a response-directed switch from nilotinib to imatinib after 12 months in patients newly diagnosed with chronic phase CML. Thirteen adult patients were enrolled. Twelve patients started on nilotinib 300 mg twice daily. Eleven patients completed one year of nilotinib and were switched to imatinib 400 mg daily as per protocol. At 3 months, all patients achieved a complete hematologic response, with 7 (58%) patients had early molecular response. At 12 months, all patients achieved CCyR, of whom 5 (42%) and 4 (33%) patients achieved MMR and MR4.5, respectively. Three (27%) patients switched back to nilotinib after 18, 24, and 51 months respectively: 1 patient because of loss of CCyR after 18 months, and 2 patients because of imatinib intolerance. At last follow-up, all patients (<i>n</i> = 12) were alive and in MMR, 6 (50%) of them in continuous MR4.5. These findings suggest that response directed switch from nilotinib to imatinib at 12 months is capable of maintaining long-term response, with manageable side effects. This approach warrants further exploration with larger prospective trials. Clinical trial registration: Clinicaltrials.gov identifier: NCT01316250, https://clinicaltrials.gov/ct2/results?cond=&term=NCT01316250&cntry=&state=&city=&dist=. .</p>","PeriodicalId":10368,"journal":{"name":"Clinical Hematology International","volume":"4 1-2","pages":"30-34"},"PeriodicalIF":0.0000,"publicationDate":"2022-05-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9358791/pdf/","citationCount":"1","resultStr":"{\"title\":\"Safety and Efficacy of Elective Switch from Nilotinib to Imatinib in Newly Diagnosed Chronic Phase Chronic Myeloid Leukemia.\",\"authors\":\"Ali Ibrahim, Nour Moukalled, Rami Mahfouz, Jean El Cheikh, Ali Bazarbachi, Iman Abou Dalle\",\"doi\":\"10.1007/s44228-022-00001-x\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>The treatment of newly diagnosed chronic phase chronic myeloid leukemia (CML) with nilotinib has resulted in a higher rate of major molecular (MMR) and complete cytogenetic response (CCyR) at 12 months compared to imatinib but at a higher cumulative cost and increased risk of serious adverse events. To maintain long-term efficacy and minimize both toxicity and costs, we aimed at evaluating in a prospective single-center trial the efficacy and safety of a response-directed switch from nilotinib to imatinib after 12 months in patients newly diagnosed with chronic phase CML. Thirteen adult patients were enrolled. Twelve patients started on nilotinib 300 mg twice daily. Eleven patients completed one year of nilotinib and were switched to imatinib 400 mg daily as per protocol. At 3 months, all patients achieved a complete hematologic response, with 7 (58%) patients had early molecular response. At 12 months, all patients achieved CCyR, of whom 5 (42%) and 4 (33%) patients achieved MMR and MR4.5, respectively. Three (27%) patients switched back to nilotinib after 18, 24, and 51 months respectively: 1 patient because of loss of CCyR after 18 months, and 2 patients because of imatinib intolerance. At last follow-up, all patients (<i>n</i> = 12) were alive and in MMR, 6 (50%) of them in continuous MR4.5. These findings suggest that response directed switch from nilotinib to imatinib at 12 months is capable of maintaining long-term response, with manageable side effects. This approach warrants further exploration with larger prospective trials. Clinical trial registration: Clinicaltrials.gov identifier: NCT01316250, https://clinicaltrials.gov/ct2/results?cond=&term=NCT01316250&cntry=&state=&city=&dist=. .</p>\",\"PeriodicalId\":10368,\"journal\":{\"name\":\"Clinical Hematology International\",\"volume\":\"4 1-2\",\"pages\":\"30-34\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2022-05-12\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9358791/pdf/\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical Hematology International\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1007/s44228-022-00001-x\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2022/6/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Hematology International","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1007/s44228-022-00001-x","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/6/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Safety and Efficacy of Elective Switch from Nilotinib to Imatinib in Newly Diagnosed Chronic Phase Chronic Myeloid Leukemia.
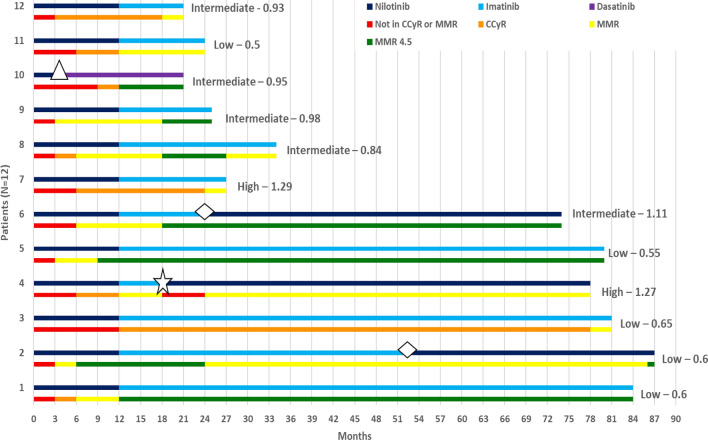
The treatment of newly diagnosed chronic phase chronic myeloid leukemia (CML) with nilotinib has resulted in a higher rate of major molecular (MMR) and complete cytogenetic response (CCyR) at 12 months compared to imatinib but at a higher cumulative cost and increased risk of serious adverse events. To maintain long-term efficacy and minimize both toxicity and costs, we aimed at evaluating in a prospective single-center trial the efficacy and safety of a response-directed switch from nilotinib to imatinib after 12 months in patients newly diagnosed with chronic phase CML. Thirteen adult patients were enrolled. Twelve patients started on nilotinib 300 mg twice daily. Eleven patients completed one year of nilotinib and were switched to imatinib 400 mg daily as per protocol. At 3 months, all patients achieved a complete hematologic response, with 7 (58%) patients had early molecular response. At 12 months, all patients achieved CCyR, of whom 5 (42%) and 4 (33%) patients achieved MMR and MR4.5, respectively. Three (27%) patients switched back to nilotinib after 18, 24, and 51 months respectively: 1 patient because of loss of CCyR after 18 months, and 2 patients because of imatinib intolerance. At last follow-up, all patients (n = 12) were alive and in MMR, 6 (50%) of them in continuous MR4.5. These findings suggest that response directed switch from nilotinib to imatinib at 12 months is capable of maintaining long-term response, with manageable side effects. This approach warrants further exploration with larger prospective trials. Clinical trial registration: Clinicaltrials.gov identifier: NCT01316250, https://clinicaltrials.gov/ct2/results?cond=&term=NCT01316250&cntry=&state=&city=&dist=. .


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
