Ingeborg Hartz, Solveig Sakshaug, Kari Furu, Anders Engeland, Anne Elise Eggen, Inger Njølstad, Svetlana Skurtveit
{"title":"他汀类药物高、平均和低消费量的挪威县的他汀类药物处方方面——一项个人水平的处方数据库研究。","authors":"Ingeborg Hartz, Solveig Sakshaug, Kari Furu, Anders Engeland, Anne Elise Eggen, Inger Njølstad, Svetlana Skurtveit","doi":"10.1186/1472-6904-7-14","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>A previous study has shown that variations in threshold and intensity (lipid goal attainment) of statins for primary prevention contribute to regional differences in overall consumption of statins in Norway. Our objective was to explore how differences in prevalences of use, dosing characteristics, choice of statin and continuity of therapy in individual patients adds new information to previous results.</p><p><strong>Methods: </strong>Data were retrieved from The Norwegian Prescription Database. We included individuals from counties with high, average, and low statin consumption, who had at least one statin prescription dispensed during 2004 (N = 40 143).1-year prevalence, prescribed daily dose (PDD), statin of choice, and continuity of therapy assessed by mean number of tablets per day.</p><p><strong>Results: </strong>The high-consumption county had higher prevalence of statin use in all age groups. Atorvastatin and simvastatin were dispensed in 79-87% of all statin users, and the proportion was significantly higher in the high-consumption county. The estimated PDDs were higher than the DDDs, up to twice the DDD for atorvastatin. The high-consumption county had the highest PDD for simvastatin (25.9 mg) and atorvastatin (21.9 mg), and more users received tablets in the upper range of available strengths. Continuity of therapy was similar in the three counties.</p><p><strong>Conclusion: </strong>Although differences in age-distribution seems to be an important source of variation in statin consumption, it cannot account for the total variation between counties in Norway. Variations in prevalences of use, and treatment intensity in terms of PDD and choice of statin also affect the total consumption. The results in this study seems to correspond to previous findings of more frequent statin use in primary prevention, and more statin users achieving lipid goal in the highest consuming county.</p>","PeriodicalId":9196,"journal":{"name":"BMC Clinical Pharmacology","volume":" ","pages":"14"},"PeriodicalIF":0.0000,"publicationDate":"2007-12-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1186/1472-6904-7-14","citationCount":"39","resultStr":"{\"title\":\"Aspects of statin prescribing in Norwegian counties with high, average and low statin consumption - an individual-level prescription database study.\",\"authors\":\"Ingeborg Hartz, Solveig Sakshaug, Kari Furu, Anders Engeland, Anne Elise Eggen, Inger Njølstad, Svetlana Skurtveit\",\"doi\":\"10.1186/1472-6904-7-14\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>A previous study has shown that variations in threshold and intensity (lipid goal attainment) of statins for primary prevention contribute to regional differences in overall consumption of statins in Norway. Our objective was to explore how differences in prevalences of use, dosing characteristics, choice of statin and continuity of therapy in individual patients adds new information to previous results.</p><p><strong>Methods: </strong>Data were retrieved from The Norwegian Prescription Database. We included individuals from counties with high, average, and low statin consumption, who had at least one statin prescription dispensed during 2004 (N = 40 143).1-year prevalence, prescribed daily dose (PDD), statin of choice, and continuity of therapy assessed by mean number of tablets per day.</p><p><strong>Results: </strong>The high-consumption county had higher prevalence of statin use in all age groups. Atorvastatin and simvastatin were dispensed in 79-87% of all statin users, and the proportion was significantly higher in the high-consumption county. The estimated PDDs were higher than the DDDs, up to twice the DDD for atorvastatin. The high-consumption county had the highest PDD for simvastatin (25.9 mg) and atorvastatin (21.9 mg), and more users received tablets in the upper range of available strengths. Continuity of therapy was similar in the three counties.</p><p><strong>Conclusion: </strong>Although differences in age-distribution seems to be an important source of variation in statin consumption, it cannot account for the total variation between counties in Norway. Variations in prevalences of use, and treatment intensity in terms of PDD and choice of statin also affect the total consumption. The results in this study seems to correspond to previous findings of more frequent statin use in primary prevention, and more statin users achieving lipid goal in the highest consuming county.</p>\",\"PeriodicalId\":9196,\"journal\":{\"name\":\"BMC Clinical Pharmacology\",\"volume\":\" \",\"pages\":\"14\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2007-12-05\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1186/1472-6904-7-14\",\"citationCount\":\"39\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"BMC Clinical Pharmacology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/1472-6904-7-14\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMC Clinical Pharmacology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/1472-6904-7-14","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Aspects of statin prescribing in Norwegian counties with high, average and low statin consumption - an individual-level prescription database study.
Background: A previous study has shown that variations in threshold and intensity (lipid goal attainment) of statins for primary prevention contribute to regional differences in overall consumption of statins in Norway. Our objective was to explore how differences in prevalences of use, dosing characteristics, choice of statin and continuity of therapy in individual patients adds new information to previous results.
Methods: Data were retrieved from The Norwegian Prescription Database. We included individuals from counties with high, average, and low statin consumption, who had at least one statin prescription dispensed during 2004 (N = 40 143).1-year prevalence, prescribed daily dose (PDD), statin of choice, and continuity of therapy assessed by mean number of tablets per day.
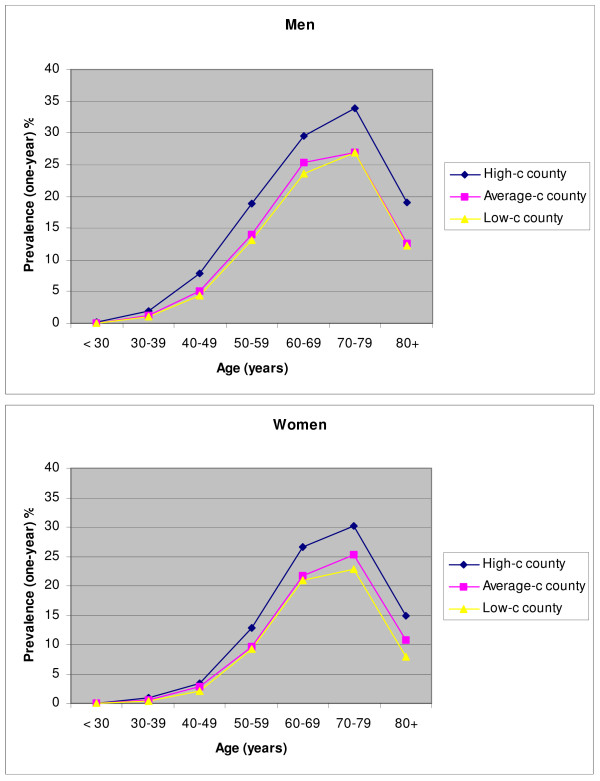
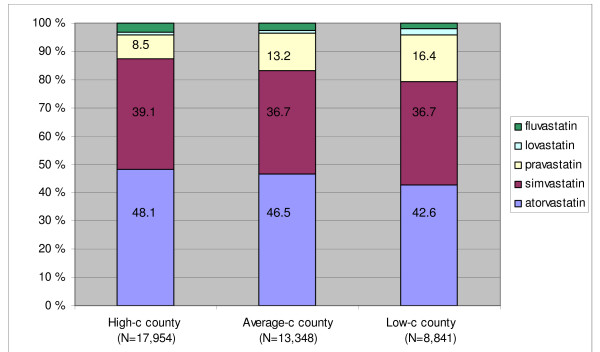
Results: The high-consumption county had higher prevalence of statin use in all age groups. Atorvastatin and simvastatin were dispensed in 79-87% of all statin users, and the proportion was significantly higher in the high-consumption county. The estimated PDDs were higher than the DDDs, up to twice the DDD for atorvastatin. The high-consumption county had the highest PDD for simvastatin (25.9 mg) and atorvastatin (21.9 mg), and more users received tablets in the upper range of available strengths. Continuity of therapy was similar in the three counties.
Conclusion: Although differences in age-distribution seems to be an important source of variation in statin consumption, it cannot account for the total variation between counties in Norway. Variations in prevalences of use, and treatment intensity in terms of PDD and choice of statin also affect the total consumption. The results in this study seems to correspond to previous findings of more frequent statin use in primary prevention, and more statin users achieving lipid goal in the highest consuming county.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
