Bassant Abdelhamid, Marina Matta, Ashraf Rady, George Adel, Medhat Gamal
{"title":"在俯卧位接受脊柱手术的患者中,传统的液体管理与基于体积描记变异指数的目标导向液体管理——一项随机对照试验。","authors":"Bassant Abdelhamid, Marina Matta, Ashraf Rady, George Adel, Medhat Gamal","doi":"10.5114/ait.2023.130792","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>The plethysmographic variability index (PVI) is a dynamic approach for assessing volume status. This study aims to compare conventional fluid management and PVI based goal-directed fluid management (GDFM) during elective spine surgery in the prone position.</p><p><strong>Material and methods: </strong>Sixty-six adult patients, ASA I-II, scheduled for elective lumbar spine procedures under general anaesthesia in the prone position were included. Patients were randomly divided into either the Conventional Group with the conventional fluid management protocol or the PVI Group with the PVI-based GDFM protocol. The total amount of intraoperative crystalloid administered was set as a primary outcome. Intraoperative PVI and perfusion index (PI), mean arterial pressure (MAP), heart rate (HR), the incidence of hypotension after prone positioning in both groups and data from arterial blood gas samples (immediately after induction of anaesthesia [T1] and immediately postoperatively [T2]) were set as secondary outcomes.</p><p><strong>Results: </strong>The total amount of intraoperative crystalloids, blood transfusion, urine output, and fluid balance were similar in the two groups ( P -values 0.443, 0.317 and 0.273, respectively). The perioperative MAP and HR values showed no significant differences between the two groups at all time points of measurements. The values of pH, PaO 2 , PaCO 2 , HCO 3 , lactate and haemoglobin showed no statistically significant difference between the two groups. The blood lactate value at T2 was significantly increased when compared to T1 values in the two groups.</p><p><strong>Conclusions: </strong>PVI dependent goal-directed fluid management (GDFM) therapy did not reduce the intraoperative total crystalloid administration or requirements for blood transfusion when compared to conventional fluid management using a fixed fluid rate in patients undergoing spine surgery in a prone position. Clinical trial registration: The study was registered at clinicaltrials.gov (NCT05239286).</p>","PeriodicalId":7750,"journal":{"name":"Anaesthesiology intensive therapy","volume":"55 3","pages":"186-195"},"PeriodicalIF":1.7000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/e7/41/AIT-55-51314.PMC10496101.pdf","citationCount":"0","resultStr":"{\"title\":\"Conventional fluid management versus plethysmographic variability index-based goal directed fluid management in patients undergoing spine surgery in the prone position - a randomised control trial.\",\"authors\":\"Bassant Abdelhamid, Marina Matta, Ashraf Rady, George Adel, Medhat Gamal\",\"doi\":\"10.5114/ait.2023.130792\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>The plethysmographic variability index (PVI) is a dynamic approach for assessing volume status. This study aims to compare conventional fluid management and PVI based goal-directed fluid management (GDFM) during elective spine surgery in the prone position.</p><p><strong>Material and methods: </strong>Sixty-six adult patients, ASA I-II, scheduled for elective lumbar spine procedures under general anaesthesia in the prone position were included. Patients were randomly divided into either the Conventional Group with the conventional fluid management protocol or the PVI Group with the PVI-based GDFM protocol. The total amount of intraoperative crystalloid administered was set as a primary outcome. Intraoperative PVI and perfusion index (PI), mean arterial pressure (MAP), heart rate (HR), the incidence of hypotension after prone positioning in both groups and data from arterial blood gas samples (immediately after induction of anaesthesia [T1] and immediately postoperatively [T2]) were set as secondary outcomes.</p><p><strong>Results: </strong>The total amount of intraoperative crystalloids, blood transfusion, urine output, and fluid balance were similar in the two groups ( P -values 0.443, 0.317 and 0.273, respectively). The perioperative MAP and HR values showed no significant differences between the two groups at all time points of measurements. The values of pH, PaO 2 , PaCO 2 , HCO 3 , lactate and haemoglobin showed no statistically significant difference between the two groups. The blood lactate value at T2 was significantly increased when compared to T1 values in the two groups.</p><p><strong>Conclusions: </strong>PVI dependent goal-directed fluid management (GDFM) therapy did not reduce the intraoperative total crystalloid administration or requirements for blood transfusion when compared to conventional fluid management using a fixed fluid rate in patients undergoing spine surgery in a prone position. Clinical trial registration: The study was registered at clinicaltrials.gov (NCT05239286).</p>\",\"PeriodicalId\":7750,\"journal\":{\"name\":\"Anaesthesiology intensive therapy\",\"volume\":\"55 3\",\"pages\":\"186-195\"},\"PeriodicalIF\":1.7000,\"publicationDate\":\"2023-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/e7/41/AIT-55-51314.PMC10496101.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Anaesthesiology intensive therapy\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.5114/ait.2023.130792\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"ANESTHESIOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Anaesthesiology intensive therapy","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5114/ait.2023.130792","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
Conventional fluid management versus plethysmographic variability index-based goal directed fluid management in patients undergoing spine surgery in the prone position - a randomised control trial.
Introduction: The plethysmographic variability index (PVI) is a dynamic approach for assessing volume status. This study aims to compare conventional fluid management and PVI based goal-directed fluid management (GDFM) during elective spine surgery in the prone position.
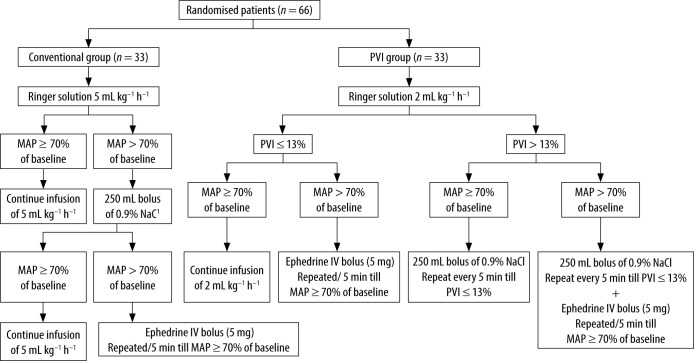
Material and methods: Sixty-six adult patients, ASA I-II, scheduled for elective lumbar spine procedures under general anaesthesia in the prone position were included. Patients were randomly divided into either the Conventional Group with the conventional fluid management protocol or the PVI Group with the PVI-based GDFM protocol. The total amount of intraoperative crystalloid administered was set as a primary outcome. Intraoperative PVI and perfusion index (PI), mean arterial pressure (MAP), heart rate (HR), the incidence of hypotension after prone positioning in both groups and data from arterial blood gas samples (immediately after induction of anaesthesia [T1] and immediately postoperatively [T2]) were set as secondary outcomes.
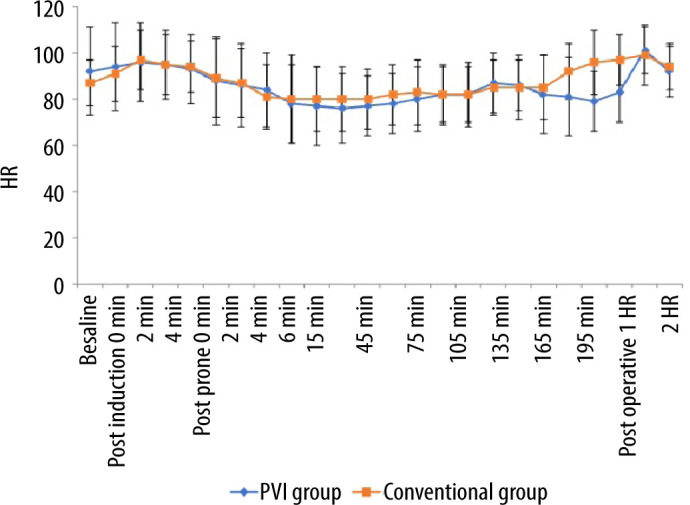
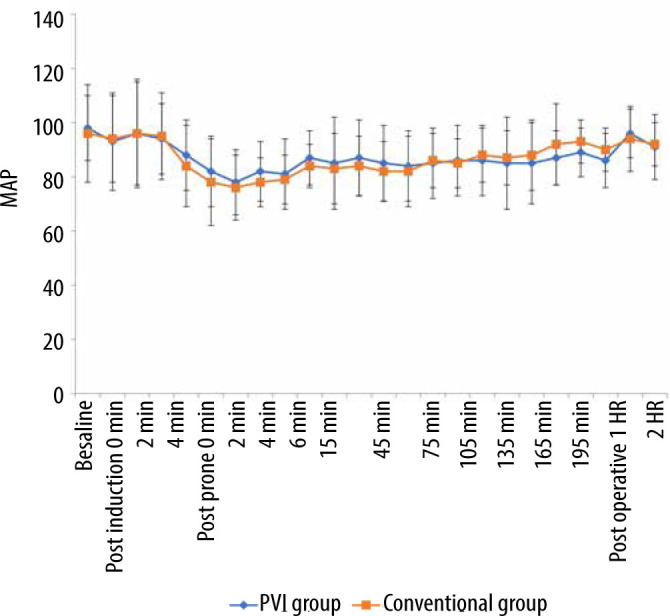
Results: The total amount of intraoperative crystalloids, blood transfusion, urine output, and fluid balance were similar in the two groups ( P -values 0.443, 0.317 and 0.273, respectively). The perioperative MAP and HR values showed no significant differences between the two groups at all time points of measurements. The values of pH, PaO 2 , PaCO 2 , HCO 3 , lactate and haemoglobin showed no statistically significant difference between the two groups. The blood lactate value at T2 was significantly increased when compared to T1 values in the two groups.
Conclusions: PVI dependent goal-directed fluid management (GDFM) therapy did not reduce the intraoperative total crystalloid administration or requirements for blood transfusion when compared to conventional fluid management using a fixed fluid rate in patients undergoing spine surgery in a prone position. Clinical trial registration: The study was registered at clinicaltrials.gov (NCT05239286).




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
