Caroline Kelley Geiger, Daniel Sheinson, Tu My To, David Jones, Nicole Gidaya Bonine
{"title":"新诊断的多发性硬化症患者按种族和民族划分的治疗模式。","authors":"Caroline Kelley Geiger, Daniel Sheinson, Tu My To, David Jones, Nicole Gidaya Bonine","doi":"10.1007/s40801-023-00387-x","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Non-Hispanic Black and Hispanic persons with MS (pwMS) are more likely to experience rapid disease progression and severe disability than non-Hispanic White pwMS; however, it is unknown how the initiation of high-efficacy disease-modifying therapies (DMTs) differs by race/ethnicity. This real-world study describes DMT treatment patterns in newly diagnosed pwMS in the United States (US) overall and by race/ethnicity.</p><p><strong>Methods: </strong>This retrospective analysis used the US Optum Market Clarity claims/electronic health records database (January 2015-September 2020). pwMS who were first diagnosed in 2016 or later and initiated any DMT in the two years following diagnosis were included. Continuous enrollment in the claims data for ≥ 12 months before and ≥ 24 months after diagnosis was required. Treatment patterns 2 years after diagnosis were analyzed descriptively overall and by race/ethnicity.</p><p><strong>Results: </strong>The sample included 682 newly diagnosed and treated pwMS (non-Hispanic Black, n = 99; non-Hispanic White, n = 479; Hispanic, n = 35; other/unknown race/ethnicity, n = 69). The mean time from diagnosis to DMT initiation was 4.9 months in all pwMS. Glatiramer acetate and dimethyl fumarate were the most common first-line DMTs in non-Hispanic Black (28% and 20% respectively) and Hispanic pwMS (31%, 29%); however, glatiramer acetate and ocrelizumab were the most common in non-Hispanic White pwMS (33%, 18%). Use of first-line high-efficacy DMTs was limited across all race/ethnicity subgroups (11-29%), but uptake increased in non-Hispanic Black and White pwMS over the study period.</p><p><strong>Conclusion: </strong>Use of high-efficacy DMTs was low across all race/ethnicity subgroups of newly diagnosed pwMS in the US, including populations at a greater risk of experiencing rapid disease progression and severe disability.</p>","PeriodicalId":11282,"journal":{"name":"Drugs - Real World Outcomes","volume":" ","pages":"565-575"},"PeriodicalIF":1.9000,"publicationDate":"2023-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10730787/pdf/","citationCount":"0","resultStr":"{\"title\":\"Treatment Patterns by Race and Ethnicity in Newly Diagnosed Persons with Multiple Sclerosis.\",\"authors\":\"Caroline Kelley Geiger, Daniel Sheinson, Tu My To, David Jones, Nicole Gidaya Bonine\",\"doi\":\"10.1007/s40801-023-00387-x\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Non-Hispanic Black and Hispanic persons with MS (pwMS) are more likely to experience rapid disease progression and severe disability than non-Hispanic White pwMS; however, it is unknown how the initiation of high-efficacy disease-modifying therapies (DMTs) differs by race/ethnicity. This real-world study describes DMT treatment patterns in newly diagnosed pwMS in the United States (US) overall and by race/ethnicity.</p><p><strong>Methods: </strong>This retrospective analysis used the US Optum Market Clarity claims/electronic health records database (January 2015-September 2020). pwMS who were first diagnosed in 2016 or later and initiated any DMT in the two years following diagnosis were included. Continuous enrollment in the claims data for ≥ 12 months before and ≥ 24 months after diagnosis was required. Treatment patterns 2 years after diagnosis were analyzed descriptively overall and by race/ethnicity.</p><p><strong>Results: </strong>The sample included 682 newly diagnosed and treated pwMS (non-Hispanic Black, n = 99; non-Hispanic White, n = 479; Hispanic, n = 35; other/unknown race/ethnicity, n = 69). The mean time from diagnosis to DMT initiation was 4.9 months in all pwMS. Glatiramer acetate and dimethyl fumarate were the most common first-line DMTs in non-Hispanic Black (28% and 20% respectively) and Hispanic pwMS (31%, 29%); however, glatiramer acetate and ocrelizumab were the most common in non-Hispanic White pwMS (33%, 18%). Use of first-line high-efficacy DMTs was limited across all race/ethnicity subgroups (11-29%), but uptake increased in non-Hispanic Black and White pwMS over the study period.</p><p><strong>Conclusion: </strong>Use of high-efficacy DMTs was low across all race/ethnicity subgroups of newly diagnosed pwMS in the US, including populations at a greater risk of experiencing rapid disease progression and severe disability.</p>\",\"PeriodicalId\":11282,\"journal\":{\"name\":\"Drugs - Real World Outcomes\",\"volume\":\" \",\"pages\":\"565-575\"},\"PeriodicalIF\":1.9000,\"publicationDate\":\"2023-12-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10730787/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Drugs - Real World Outcomes\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1007/s40801-023-00387-x\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/9/21 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"PHARMACOLOGY & PHARMACY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Drugs - Real World Outcomes","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1007/s40801-023-00387-x","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/9/21 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"PHARMACOLOGY & PHARMACY","Score":null,"Total":0}
Treatment Patterns by Race and Ethnicity in Newly Diagnosed Persons with Multiple Sclerosis.
Background: Non-Hispanic Black and Hispanic persons with MS (pwMS) are more likely to experience rapid disease progression and severe disability than non-Hispanic White pwMS; however, it is unknown how the initiation of high-efficacy disease-modifying therapies (DMTs) differs by race/ethnicity. This real-world study describes DMT treatment patterns in newly diagnosed pwMS in the United States (US) overall and by race/ethnicity.
Methods: This retrospective analysis used the US Optum Market Clarity claims/electronic health records database (January 2015-September 2020). pwMS who were first diagnosed in 2016 or later and initiated any DMT in the two years following diagnosis were included. Continuous enrollment in the claims data for ≥ 12 months before and ≥ 24 months after diagnosis was required. Treatment patterns 2 years after diagnosis were analyzed descriptively overall and by race/ethnicity.
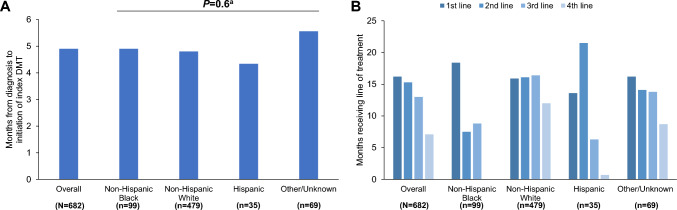
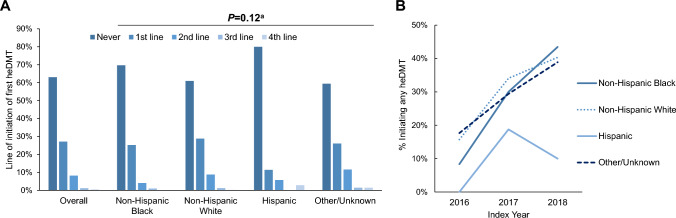
Results: The sample included 682 newly diagnosed and treated pwMS (non-Hispanic Black, n = 99; non-Hispanic White, n = 479; Hispanic, n = 35; other/unknown race/ethnicity, n = 69). The mean time from diagnosis to DMT initiation was 4.9 months in all pwMS. Glatiramer acetate and dimethyl fumarate were the most common first-line DMTs in non-Hispanic Black (28% and 20% respectively) and Hispanic pwMS (31%, 29%); however, glatiramer acetate and ocrelizumab were the most common in non-Hispanic White pwMS (33%, 18%). Use of first-line high-efficacy DMTs was limited across all race/ethnicity subgroups (11-29%), but uptake increased in non-Hispanic Black and White pwMS over the study period.
Conclusion: Use of high-efficacy DMTs was low across all race/ethnicity subgroups of newly diagnosed pwMS in the US, including populations at a greater risk of experiencing rapid disease progression and severe disability.
期刊介绍:
Drugs - Real World Outcomes targets original research and definitive reviews regarding the use of real-world data to evaluate health outcomes and inform healthcare decision-making on drugs, devices and other interventions in clinical practice. The journal includes, but is not limited to, the following research areas: Using registries/databases/health records and other non-selected observational datasets to investigate: drug use and treatment outcomes prescription patterns drug safety signals adherence to treatment guidelines benefit : risk profiles comparative effectiveness economic analyses including cost-of-illness Data-driven research methodologies, including the capture, curation, search, sharing, analysis and interpretation of ‘big data’ Techniques and approaches to optimise real-world modelling.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
