Casper Falster, Amanda Juul, Niels Jacobsen, Inge Raadal Skov, Line Dahlerup Rasmussen, Lone Wulff Madsen, Isik Somuncu Johansen, Stefan Markus Walbom Harders Harders, Jesper Rømhild Davidsen, Christian B Laursen
{"title":"新冠肺炎患者12个月随访时的胸部超声和临床表现。","authors":"Casper Falster, Amanda Juul, Niels Jacobsen, Inge Raadal Skov, Line Dahlerup Rasmussen, Lone Wulff Madsen, Isik Somuncu Johansen, Stefan Markus Walbom Harders Harders, Jesper Rømhild Davidsen, Christian B Laursen","doi":"10.1080/20018525.2023.2257992","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Thoracic ultrasound (TUS) has proven useful in the diagnosis, risk stratification and monitoring of disease progression in patients with coronavirus disease 2019 (COVID-19). However, utility in follow-up is poorly described. To elucidate this area, we performed TUS as part of a 12-month clinical follow-up in patients previously admitted with COVID-19 and correlated findings with clinical assessment and pulmonary function tests.</p><p><strong>Methods: </strong>Adult patients discharged from our hospital following admission with COVID-19 during March to May 2020 were invited to a 12-month follow-up. Enrolled patients were interviewed regarding persisting or newly developed symptoms in addition to TUS, spirometry and a 6-min walk test. Patients were referred to high-resolution computed tomography (HRCT) of the lungs if suspicion of pulmonary fibrosis was raised.</p><p><strong>Results: </strong>Forty patients were enrolled in the study of whom had 13 developed acute respiratory distress syndrome (ARDS) during admission. Patients with ARDS were more prone to experience neurological symptoms at follow-up (<i>p</i> = 0.03) and showed more B-lines on TUS (<i>p</i> = 0.008) but did not otherwise differ significantly in terms of pulmonary function tests. Four patients had pathological findings on TUS where subsequent diagnostics revealed that two had interstitial lung abnormalities and two had heart failure. These four patients presented with a significantly lower diffusing capacity of lung for carbon monoxide (<i>p</i>=0.03) and 6-min walking distance (<i>p</i>=0.006) compared to the remaining 36 patients without ultrasound pathology. No significant difference was observed in spirometry values of % of predicted FEV1 (<i>p</i>=0.49) or FVC (<i>p</i>=0.07). No persisting cardiovascular pathology was observed in patients without ultrasonographic pathology.</p><p><strong>Conclusion: </strong>At 12-month after admission with COVID-19, a follow-up combining TUS, clinical assessment, and pulmonary function tests may improve the selection of patients requiring further diagnostic investigations such as HRCT or echocardiography.</p>","PeriodicalId":11872,"journal":{"name":"European Clinical Respiratory Journal","volume":"10 1","pages":"2257992"},"PeriodicalIF":1.4000,"publicationDate":"2023-09-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/7f/62/ZECR_10_2257992.PMC10519251.pdf","citationCount":"0","resultStr":"{\"title\":\"Thoracic ultrasonographic and clinical findings at 12-month follow-up of patients admitted with COVID-19.\",\"authors\":\"Casper Falster, Amanda Juul, Niels Jacobsen, Inge Raadal Skov, Line Dahlerup Rasmussen, Lone Wulff Madsen, Isik Somuncu Johansen, Stefan Markus Walbom Harders Harders, Jesper Rømhild Davidsen, Christian B Laursen\",\"doi\":\"10.1080/20018525.2023.2257992\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Thoracic ultrasound (TUS) has proven useful in the diagnosis, risk stratification and monitoring of disease progression in patients with coronavirus disease 2019 (COVID-19). However, utility in follow-up is poorly described. To elucidate this area, we performed TUS as part of a 12-month clinical follow-up in patients previously admitted with COVID-19 and correlated findings with clinical assessment and pulmonary function tests.</p><p><strong>Methods: </strong>Adult patients discharged from our hospital following admission with COVID-19 during March to May 2020 were invited to a 12-month follow-up. Enrolled patients were interviewed regarding persisting or newly developed symptoms in addition to TUS, spirometry and a 6-min walk test. Patients were referred to high-resolution computed tomography (HRCT) of the lungs if suspicion of pulmonary fibrosis was raised.</p><p><strong>Results: </strong>Forty patients were enrolled in the study of whom had 13 developed acute respiratory distress syndrome (ARDS) during admission. Patients with ARDS were more prone to experience neurological symptoms at follow-up (<i>p</i> = 0.03) and showed more B-lines on TUS (<i>p</i> = 0.008) but did not otherwise differ significantly in terms of pulmonary function tests. Four patients had pathological findings on TUS where subsequent diagnostics revealed that two had interstitial lung abnormalities and two had heart failure. These four patients presented with a significantly lower diffusing capacity of lung for carbon monoxide (<i>p</i>=0.03) and 6-min walking distance (<i>p</i>=0.006) compared to the remaining 36 patients without ultrasound pathology. No significant difference was observed in spirometry values of % of predicted FEV1 (<i>p</i>=0.49) or FVC (<i>p</i>=0.07). No persisting cardiovascular pathology was observed in patients without ultrasonographic pathology.</p><p><strong>Conclusion: </strong>At 12-month after admission with COVID-19, a follow-up combining TUS, clinical assessment, and pulmonary function tests may improve the selection of patients requiring further diagnostic investigations such as HRCT or echocardiography.</p>\",\"PeriodicalId\":11872,\"journal\":{\"name\":\"European Clinical Respiratory Journal\",\"volume\":\"10 1\",\"pages\":\"2257992\"},\"PeriodicalIF\":1.4000,\"publicationDate\":\"2023-09-24\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/7f/62/ZECR_10_2257992.PMC10519251.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"European Clinical Respiratory Journal\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1080/20018525.2023.2257992\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"RESPIRATORY SYSTEM\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"European Clinical Respiratory Journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1080/20018525.2023.2257992","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
Thoracic ultrasonographic and clinical findings at 12-month follow-up of patients admitted with COVID-19.
Introduction: Thoracic ultrasound (TUS) has proven useful in the diagnosis, risk stratification and monitoring of disease progression in patients with coronavirus disease 2019 (COVID-19). However, utility in follow-up is poorly described. To elucidate this area, we performed TUS as part of a 12-month clinical follow-up in patients previously admitted with COVID-19 and correlated findings with clinical assessment and pulmonary function tests.
Methods: Adult patients discharged from our hospital following admission with COVID-19 during March to May 2020 were invited to a 12-month follow-up. Enrolled patients were interviewed regarding persisting or newly developed symptoms in addition to TUS, spirometry and a 6-min walk test. Patients were referred to high-resolution computed tomography (HRCT) of the lungs if suspicion of pulmonary fibrosis was raised.
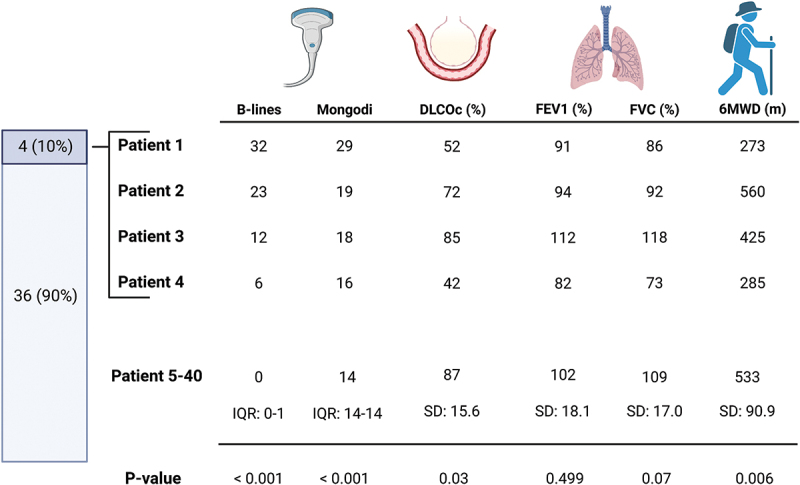
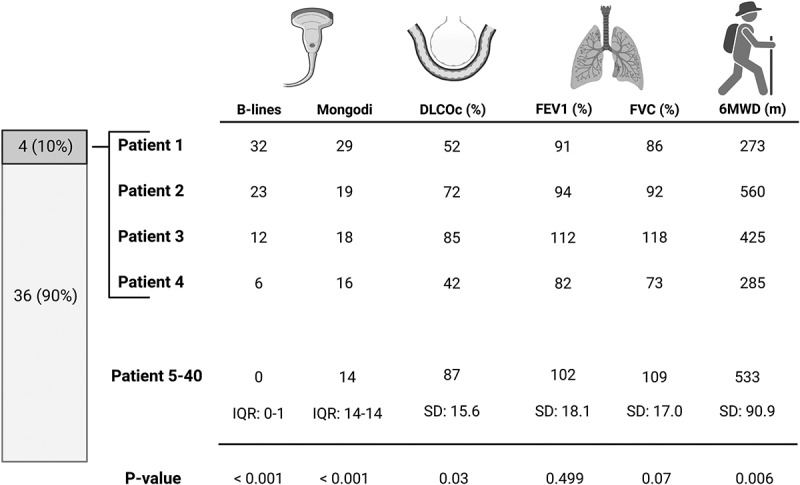
Results: Forty patients were enrolled in the study of whom had 13 developed acute respiratory distress syndrome (ARDS) during admission. Patients with ARDS were more prone to experience neurological symptoms at follow-up (p = 0.03) and showed more B-lines on TUS (p = 0.008) but did not otherwise differ significantly in terms of pulmonary function tests. Four patients had pathological findings on TUS where subsequent diagnostics revealed that two had interstitial lung abnormalities and two had heart failure. These four patients presented with a significantly lower diffusing capacity of lung for carbon monoxide (p=0.03) and 6-min walking distance (p=0.006) compared to the remaining 36 patients without ultrasound pathology. No significant difference was observed in spirometry values of % of predicted FEV1 (p=0.49) or FVC (p=0.07). No persisting cardiovascular pathology was observed in patients without ultrasonographic pathology.
Conclusion: At 12-month after admission with COVID-19, a follow-up combining TUS, clinical assessment, and pulmonary function tests may improve the selection of patients requiring further diagnostic investigations such as HRCT or echocardiography.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
