Bethany Forseth, Adrian Ortega, Paul R Hibbing, Mallory Moon, Chelsea Steel, A Singh, Avinash Kollu, Bryce Miller, Maurice Miller, Vincent Staggs, Hannah Calvert, Ann M Davis, Jordan Carlson
{"title":"将家庭数字支持添加到基于教室的体育活动干预中,以针对校内和校外活动:新冠肺炎大流行期间保持积极干预的评估。","authors":"Bethany Forseth, Adrian Ortega, Paul R Hibbing, Mallory Moon, Chelsea Steel, A Singh, Avinash Kollu, Bryce Miller, Maurice Miller, Vincent Staggs, Hannah Calvert, Ann M Davis, Jordan Carlson","doi":"","DOIUrl":null,"url":null,"abstract":"<p><p>Remotely delivered interventions are promising for reaching large numbers of people, though few have targeted multiple levels of influence such as schools and families. This study evaluated two versions (arms) of a remotely delivered classroom-based physical activity (CBPA) intervention. One arm solely included remote CBPA; the other included remote CBPA and mobile health (mHealth) family supports. Six schools were randomized to CBPA or CBPA+Family. Both arms were remotely delivered for seven weeks. CBPA+Family added behavior change tools delivered via text messages and newsletters to caregiver/child dyads. Garmin devices measured moderate-to-vigorous activity (MVPA) in both arms and were used for goal setting/ monitoring in the CBPA+Family arm (integrated with the text messages). Caregivers completed surveys evaluating intervention acceptability. 53 participants (CBPA n=35; CBPA+Family n=18; 9.7±0.7 years) were included. Increases in MVPA were similar between arms, showing a pre-post effect of the CBPA but no additional effect of family supports. MVPA was low at baseline and during the first 3 weeks (CBPA 7.5±3.1 minutes/day; CBPA+Family 7.9±2.7 minutes/day) and increased by Weeks 6-8 (CBPA 56.8±34.2 minutes/day; CBPA+Family 49.2±18.7 minutes/day). Approximately 90% of caregivers reported high satisfaction with the added family support content. CBPA+Family participants wore the Garmin later into the study period. Remote delivery of CBPA appears feasible and effective for supporting increases in children's MVPA. Adding family supports to school-based interventions appears acceptable and may support engagement, demonstrating promise for more multilevel/multi-setting interventions, though the multilevel intervention was not more effective than the single-level intervention in increasing children's MVPA.</p>","PeriodicalId":73774,"journal":{"name":"Journal of healthy eating and active living","volume":"1 4","pages":"226-240"},"PeriodicalIF":0.0000,"publicationDate":"2021-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/f2/f8/jheal-1-4-226.PMC10522008.pdf","citationCount":"0","resultStr":"{\"title\":\"Adding Family Digital Supports to Classroom-Based Physical Activity Interventions to Target In- and Out-of-School Activity: An Evaluation of the Stay Active Intervention during the COVID-19 Pandemic.\",\"authors\":\"Bethany Forseth, Adrian Ortega, Paul R Hibbing, Mallory Moon, Chelsea Steel, A Singh, Avinash Kollu, Bryce Miller, Maurice Miller, Vincent Staggs, Hannah Calvert, Ann M Davis, Jordan Carlson\",\"doi\":\"\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Remotely delivered interventions are promising for reaching large numbers of people, though few have targeted multiple levels of influence such as schools and families. This study evaluated two versions (arms) of a remotely delivered classroom-based physical activity (CBPA) intervention. One arm solely included remote CBPA; the other included remote CBPA and mobile health (mHealth) family supports. Six schools were randomized to CBPA or CBPA+Family. Both arms were remotely delivered for seven weeks. CBPA+Family added behavior change tools delivered via text messages and newsletters to caregiver/child dyads. Garmin devices measured moderate-to-vigorous activity (MVPA) in both arms and were used for goal setting/ monitoring in the CBPA+Family arm (integrated with the text messages). Caregivers completed surveys evaluating intervention acceptability. 53 participants (CBPA n=35; CBPA+Family n=18; 9.7±0.7 years) were included. Increases in MVPA were similar between arms, showing a pre-post effect of the CBPA but no additional effect of family supports. MVPA was low at baseline and during the first 3 weeks (CBPA 7.5±3.1 minutes/day; CBPA+Family 7.9±2.7 minutes/day) and increased by Weeks 6-8 (CBPA 56.8±34.2 minutes/day; CBPA+Family 49.2±18.7 minutes/day). Approximately 90% of caregivers reported high satisfaction with the added family support content. CBPA+Family participants wore the Garmin later into the study period. Remote delivery of CBPA appears feasible and effective for supporting increases in children's MVPA. Adding family supports to school-based interventions appears acceptable and may support engagement, demonstrating promise for more multilevel/multi-setting interventions, though the multilevel intervention was not more effective than the single-level intervention in increasing children's MVPA.</p>\",\"PeriodicalId\":73774,\"journal\":{\"name\":\"Journal of healthy eating and active living\",\"volume\":\"1 4\",\"pages\":\"226-240\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2021-12-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/f2/f8/jheal-1-4-226.PMC10522008.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of healthy eating and active living\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2021/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of healthy eating and active living","FirstCategoryId":"1085","ListUrlMain":"","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Adding Family Digital Supports to Classroom-Based Physical Activity Interventions to Target In- and Out-of-School Activity: An Evaluation of the Stay Active Intervention during the COVID-19 Pandemic.
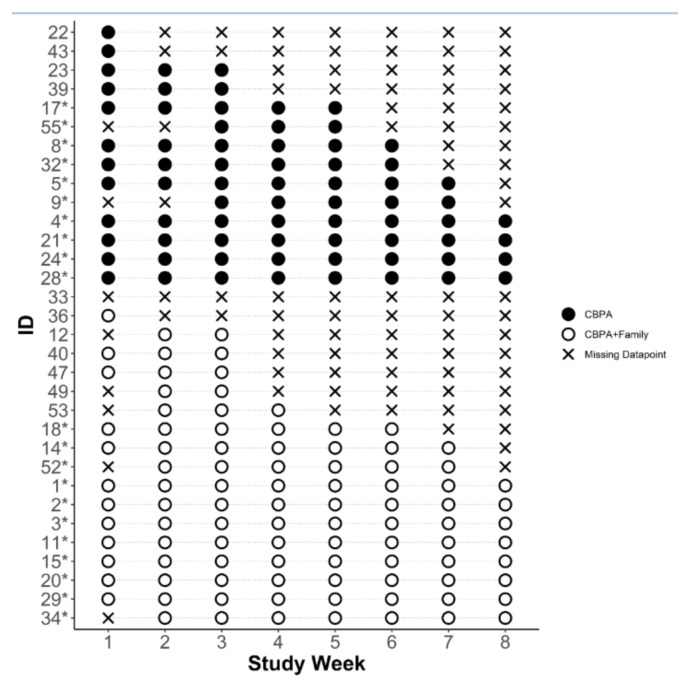
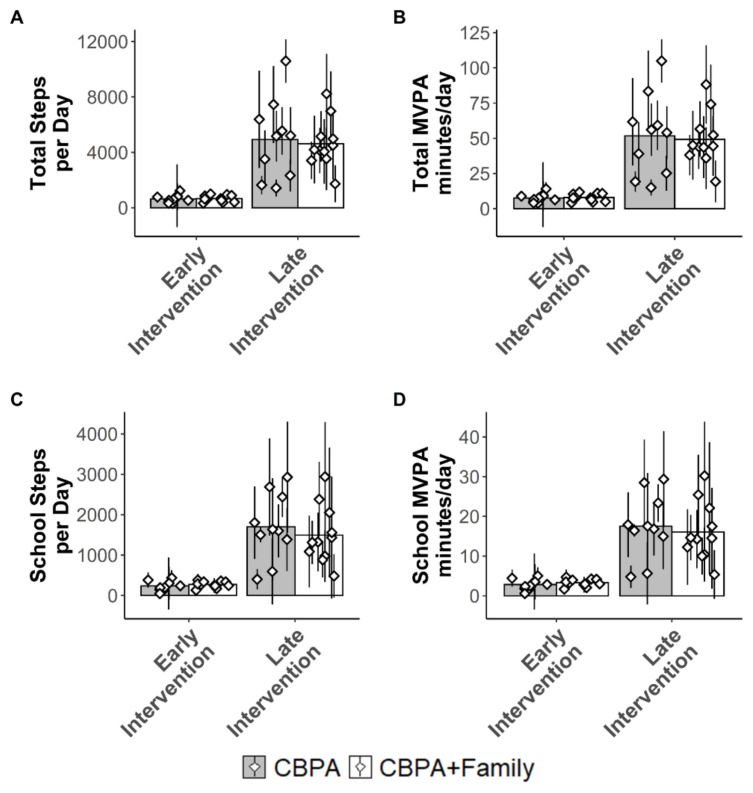
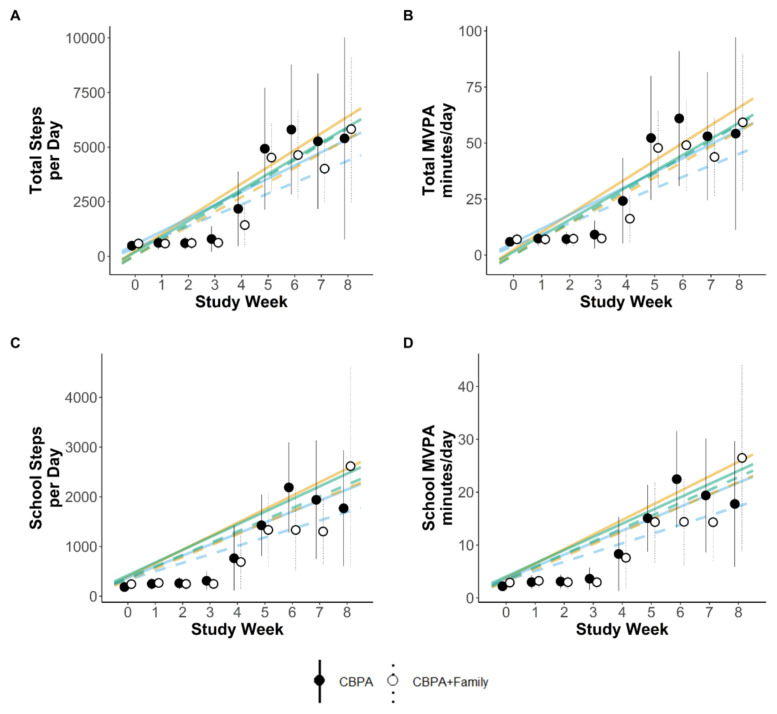
Remotely delivered interventions are promising for reaching large numbers of people, though few have targeted multiple levels of influence such as schools and families. This study evaluated two versions (arms) of a remotely delivered classroom-based physical activity (CBPA) intervention. One arm solely included remote CBPA; the other included remote CBPA and mobile health (mHealth) family supports. Six schools were randomized to CBPA or CBPA+Family. Both arms were remotely delivered for seven weeks. CBPA+Family added behavior change tools delivered via text messages and newsletters to caregiver/child dyads. Garmin devices measured moderate-to-vigorous activity (MVPA) in both arms and were used for goal setting/ monitoring in the CBPA+Family arm (integrated with the text messages). Caregivers completed surveys evaluating intervention acceptability. 53 participants (CBPA n=35; CBPA+Family n=18; 9.7±0.7 years) were included. Increases in MVPA were similar between arms, showing a pre-post effect of the CBPA but no additional effect of family supports. MVPA was low at baseline and during the first 3 weeks (CBPA 7.5±3.1 minutes/day; CBPA+Family 7.9±2.7 minutes/day) and increased by Weeks 6-8 (CBPA 56.8±34.2 minutes/day; CBPA+Family 49.2±18.7 minutes/day). Approximately 90% of caregivers reported high satisfaction with the added family support content. CBPA+Family participants wore the Garmin later into the study period. Remote delivery of CBPA appears feasible and effective for supporting increases in children's MVPA. Adding family supports to school-based interventions appears acceptable and may support engagement, demonstrating promise for more multilevel/multi-setting interventions, though the multilevel intervention was not more effective than the single-level intervention in increasing children's MVPA.
 分享
分享



 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
