Shaofu Yu, Shasha Zhai, Qian Gong, Chunhong Xiang, Jianping Gong, Lin Wu, Xingxiang Pu
{"title":"新辅助免疫治疗与非小细胞肺癌癌症:随机对照试验的系统评价和Meta-analysis。","authors":"Shaofu Yu, Shasha Zhai, Qian Gong, Chunhong Xiang, Jianping Gong, Lin Wu, Xingxiang Pu","doi":"10.1097/COC.0000000000001046","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>To systematically evaluate the effectiveness and safety of neoadjuvant immunotherapy for patients with non-small cell lung cancer (NSCLC).</p><p><strong>Methods: </strong>Randomized controlled trials of neoadjuvant immunotherapy in treating patients with NSCLC were comprehensively retrieved from electronic databases, eligible studies, previous systematic reviews and meta-analyses, guidelines, and conference abstracts. The meta-analysis was performed by the Stata/SE 12.0 software.</p><p><strong>Results: </strong>Eleven randomized controlled trials were eventually included. The results of the meta-analysis showed that neoadjuvant immunochemotherapy significantly improved the objective response rate compared with neoadjuvant chemotherapy (CT; 62.46% vs 41.88%, P = 0.003), but the objective response rate of neoadjuvant double-immunotherapy was roughly comparable to that of neoadjuvant single-immunotherapy (15.74% vs 10.45%, P = 0.387). Major pathologic response (MPR) rate and pathologic complete response (pCR) rate of neoadjuvant immunochemotherapy and neoadjuvant double-immunotherapy were significantly superior to neoadjuvant CT alone and neoadjuvant single-immunotherapy, respectively. Compared with neoadjuvant CT alone, neoadjuvant immunochemotherapy increased the down-staging rate (40.16% vs 26.70%, P = 0.060), the surgical resection rate (83.69% vs 73.07%, P = 0.231), and R0 resection rate (86.19% vs 77.98%, P = 0.502), but there were no statistically significant differences. Neoadjuvant immunochemotherapy did not increase the postoperative complications rate than neoadjuvant CT alone (40.20% vs 41.30%, P = 0.920). In terms of safety, neoadjuvant immunochemotherapy and neoadjuvant double-immunotherapy did not increase the incidence of treatment-related adverse events (TRAEs) and the grade 3 or higher TRAEs.</p><p><strong>Conclusions: </strong>In summary, neoadjuvant immunochemotherapy had better clinical efficacy than neoadjuvant CT for patients with NSCLC. MPR rate and pCR rate of neoadjuvant immunochemotherapy and neoadjuvant double-immunotherapy were significantly superior to neoadjuvant CT and neoadjuvant single-immunotherapy, respectively, for patients with NSCLC, showing that MPR rate and pCR rate were probably considered as alternative endpoints for survival benefit. TRAEs were comparable between the corresponding groups. The long-term survival outcome of neoadjuvant immunotherapy for patients with NSCLC needs to be further confirmed to better guide clinical practice.</p>","PeriodicalId":50812,"journal":{"name":"American Journal of Clinical Oncology-Cancer Clinical Trials","volume":" ","pages":"517-528"},"PeriodicalIF":1.8000,"publicationDate":"2023-11-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/fa/c4/coc-46-517.PMC10589427.pdf","citationCount":"0","resultStr":"{\"title\":\"Neoadjuvant Immunotherapy and Non-Small Cell Lung Cancer: A Systematic Review and Meta-analysis of Randomized Controlled Trials.\",\"authors\":\"Shaofu Yu, Shasha Zhai, Qian Gong, Chunhong Xiang, Jianping Gong, Lin Wu, Xingxiang Pu\",\"doi\":\"10.1097/COC.0000000000001046\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objectives: </strong>To systematically evaluate the effectiveness and safety of neoadjuvant immunotherapy for patients with non-small cell lung cancer (NSCLC).</p><p><strong>Methods: </strong>Randomized controlled trials of neoadjuvant immunotherapy in treating patients with NSCLC were comprehensively retrieved from electronic databases, eligible studies, previous systematic reviews and meta-analyses, guidelines, and conference abstracts. The meta-analysis was performed by the Stata/SE 12.0 software.</p><p><strong>Results: </strong>Eleven randomized controlled trials were eventually included. The results of the meta-analysis showed that neoadjuvant immunochemotherapy significantly improved the objective response rate compared with neoadjuvant chemotherapy (CT; 62.46% vs 41.88%, P = 0.003), but the objective response rate of neoadjuvant double-immunotherapy was roughly comparable to that of neoadjuvant single-immunotherapy (15.74% vs 10.45%, P = 0.387). Major pathologic response (MPR) rate and pathologic complete response (pCR) rate of neoadjuvant immunochemotherapy and neoadjuvant double-immunotherapy were significantly superior to neoadjuvant CT alone and neoadjuvant single-immunotherapy, respectively. Compared with neoadjuvant CT alone, neoadjuvant immunochemotherapy increased the down-staging rate (40.16% vs 26.70%, P = 0.060), the surgical resection rate (83.69% vs 73.07%, P = 0.231), and R0 resection rate (86.19% vs 77.98%, P = 0.502), but there were no statistically significant differences. Neoadjuvant immunochemotherapy did not increase the postoperative complications rate than neoadjuvant CT alone (40.20% vs 41.30%, P = 0.920). In terms of safety, neoadjuvant immunochemotherapy and neoadjuvant double-immunotherapy did not increase the incidence of treatment-related adverse events (TRAEs) and the grade 3 or higher TRAEs.</p><p><strong>Conclusions: </strong>In summary, neoadjuvant immunochemotherapy had better clinical efficacy than neoadjuvant CT for patients with NSCLC. MPR rate and pCR rate of neoadjuvant immunochemotherapy and neoadjuvant double-immunotherapy were significantly superior to neoadjuvant CT and neoadjuvant single-immunotherapy, respectively, for patients with NSCLC, showing that MPR rate and pCR rate were probably considered as alternative endpoints for survival benefit. TRAEs were comparable between the corresponding groups. The long-term survival outcome of neoadjuvant immunotherapy for patients with NSCLC needs to be further confirmed to better guide clinical practice.</p>\",\"PeriodicalId\":50812,\"journal\":{\"name\":\"American Journal of Clinical Oncology-Cancer Clinical Trials\",\"volume\":\" \",\"pages\":\"517-528\"},\"PeriodicalIF\":1.8000,\"publicationDate\":\"2023-11-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/fa/c4/coc-46-517.PMC10589427.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"American Journal of Clinical Oncology-Cancer Clinical Trials\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1097/COC.0000000000001046\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/9/26 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q4\",\"JCRName\":\"ONCOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"American Journal of Clinical Oncology-Cancer Clinical Trials","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1097/COC.0000000000001046","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/9/26 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"ONCOLOGY","Score":null,"Total":0}
Neoadjuvant Immunotherapy and Non-Small Cell Lung Cancer: A Systematic Review and Meta-analysis of Randomized Controlled Trials.
Objectives: To systematically evaluate the effectiveness and safety of neoadjuvant immunotherapy for patients with non-small cell lung cancer (NSCLC).
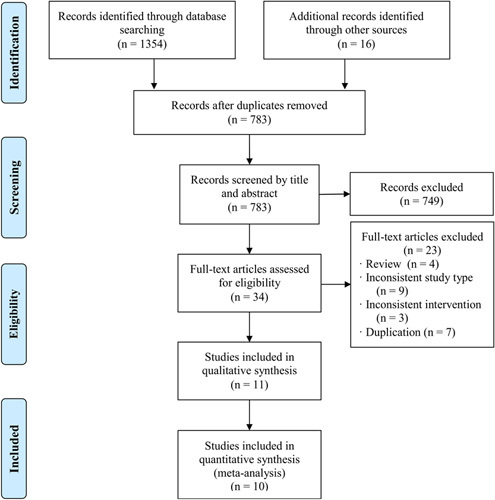
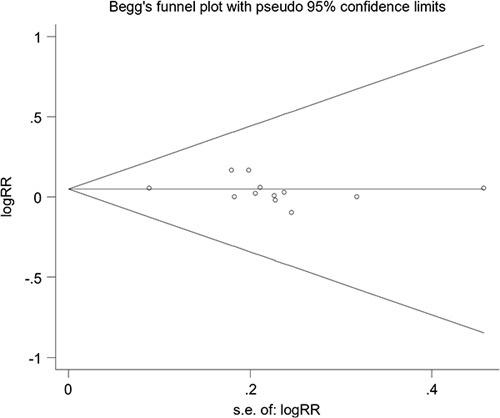
Methods: Randomized controlled trials of neoadjuvant immunotherapy in treating patients with NSCLC were comprehensively retrieved from electronic databases, eligible studies, previous systematic reviews and meta-analyses, guidelines, and conference abstracts. The meta-analysis was performed by the Stata/SE 12.0 software.
Results: Eleven randomized controlled trials were eventually included. The results of the meta-analysis showed that neoadjuvant immunochemotherapy significantly improved the objective response rate compared with neoadjuvant chemotherapy (CT; 62.46% vs 41.88%, P = 0.003), but the objective response rate of neoadjuvant double-immunotherapy was roughly comparable to that of neoadjuvant single-immunotherapy (15.74% vs 10.45%, P = 0.387). Major pathologic response (MPR) rate and pathologic complete response (pCR) rate of neoadjuvant immunochemotherapy and neoadjuvant double-immunotherapy were significantly superior to neoadjuvant CT alone and neoadjuvant single-immunotherapy, respectively. Compared with neoadjuvant CT alone, neoadjuvant immunochemotherapy increased the down-staging rate (40.16% vs 26.70%, P = 0.060), the surgical resection rate (83.69% vs 73.07%, P = 0.231), and R0 resection rate (86.19% vs 77.98%, P = 0.502), but there were no statistically significant differences. Neoadjuvant immunochemotherapy did not increase the postoperative complications rate than neoadjuvant CT alone (40.20% vs 41.30%, P = 0.920). In terms of safety, neoadjuvant immunochemotherapy and neoadjuvant double-immunotherapy did not increase the incidence of treatment-related adverse events (TRAEs) and the grade 3 or higher TRAEs.
Conclusions: In summary, neoadjuvant immunochemotherapy had better clinical efficacy than neoadjuvant CT for patients with NSCLC. MPR rate and pCR rate of neoadjuvant immunochemotherapy and neoadjuvant double-immunotherapy were significantly superior to neoadjuvant CT and neoadjuvant single-immunotherapy, respectively, for patients with NSCLC, showing that MPR rate and pCR rate were probably considered as alternative endpoints for survival benefit. TRAEs were comparable between the corresponding groups. The long-term survival outcome of neoadjuvant immunotherapy for patients with NSCLC needs to be further confirmed to better guide clinical practice.
期刊介绍:
American Journal of Clinical Oncology is a multidisciplinary journal for cancer surgeons, radiation oncologists, medical oncologists, GYN oncologists, and pediatric oncologists.
The emphasis of AJCO is on combined modality multidisciplinary loco-regional management of cancer. The journal also gives emphasis to translational research, outcome studies, and cost utility analyses, and includes opinion pieces and review articles.
The editorial board includes a large number of distinguished surgeons, radiation oncologists, medical oncologists, GYN oncologists, pediatric oncologists, and others who are internationally recognized for expertise in their fields.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
