Victoria Hamilton, Sadiyah Sheikh, Alicja Szczepanska, Nick Maskell, Fergus Hamilton, Jonathan P Reid, Bryan R Bzdek, James R D Murray
{"title":"透热和锯骨是高气溶胶产量的程序。","authors":"Victoria Hamilton, Sadiyah Sheikh, Alicja Szczepanska, Nick Maskell, Fergus Hamilton, Jonathan P Reid, Bryan R Bzdek, James R D Murray","doi":"10.1302/2046-3758.1210.BJR-2023-0028.R1","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>Orthopaedic surgery uses many varied instruments with high-speed, high-impact, thermal energy and sometimes heavy instruments, all of which potentially result in aerosolization of contaminated blood, tissue, and bone, raising concerns for clinicians' health. This study quantifies the aerosol exposure by measuring the number and size distribution of the particles reaching the lead surgeon during key orthopaedic operations.</p><p><strong>Methods: </strong>The aerosol yield from 17 orthopaedic open surgeries (on the knee, hip, and shoulder) was recorded at the position of the lead surgeon using an Aerodynamic Particle Sizer (APS; 0.5 to 20 μm diameter particles) sampling at 1 s time resolution. Through timestamping, detected aerosol was attributed to specific procedures.</p><p><strong>Results: </strong>Diathermy (electrocautery) and oscillating bone saw use had a high aerosol yield (> 100 particles detected per s) consistent with high exposure to aerosol in the respirable range (< 5 µm) for the lead surgeon. Pulsed lavage, reaming, osteotome use, and jig application/removal were medium aerosol yield (10 to 100 particles s<sup>-1</sup>). However, pulsed lavage aerosol was largely attributed to the saline jet, osteotome use was always brief, and jig application/removal had a large variability in the associated aerosol yield. Suctioning (with/without saline irrigation) had a low aerosol yield (< 10 particles s<sup>-1</sup>). Most surprisingly, other high-speed procedures, such as drilling and screwing, had low aerosol yields.</p><p><strong>Conclusion: </strong>This work suggests that additional precautions should be recommended for diathermy and bone sawing, such as enhanced personal protective equipment or the use of suction devices to reduce exposure.</p>","PeriodicalId":9074,"journal":{"name":"Bone & Joint Research","volume":"12 10","pages":"636-643"},"PeriodicalIF":4.7000,"publicationDate":"2023-10-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10562079/pdf/","citationCount":"0","resultStr":"{\"title\":\"Diathermy and bone sawing are high aerosol yield procedures.\",\"authors\":\"Victoria Hamilton, Sadiyah Sheikh, Alicja Szczepanska, Nick Maskell, Fergus Hamilton, Jonathan P Reid, Bryan R Bzdek, James R D Murray\",\"doi\":\"10.1302/2046-3758.1210.BJR-2023-0028.R1\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Aims: </strong>Orthopaedic surgery uses many varied instruments with high-speed, high-impact, thermal energy and sometimes heavy instruments, all of which potentially result in aerosolization of contaminated blood, tissue, and bone, raising concerns for clinicians' health. This study quantifies the aerosol exposure by measuring the number and size distribution of the particles reaching the lead surgeon during key orthopaedic operations.</p><p><strong>Methods: </strong>The aerosol yield from 17 orthopaedic open surgeries (on the knee, hip, and shoulder) was recorded at the position of the lead surgeon using an Aerodynamic Particle Sizer (APS; 0.5 to 20 μm diameter particles) sampling at 1 s time resolution. Through timestamping, detected aerosol was attributed to specific procedures.</p><p><strong>Results: </strong>Diathermy (electrocautery) and oscillating bone saw use had a high aerosol yield (> 100 particles detected per s) consistent with high exposure to aerosol in the respirable range (< 5 µm) for the lead surgeon. Pulsed lavage, reaming, osteotome use, and jig application/removal were medium aerosol yield (10 to 100 particles s<sup>-1</sup>). However, pulsed lavage aerosol was largely attributed to the saline jet, osteotome use was always brief, and jig application/removal had a large variability in the associated aerosol yield. Suctioning (with/without saline irrigation) had a low aerosol yield (< 10 particles s<sup>-1</sup>). Most surprisingly, other high-speed procedures, such as drilling and screwing, had low aerosol yields.</p><p><strong>Conclusion: </strong>This work suggests that additional precautions should be recommended for diathermy and bone sawing, such as enhanced personal protective equipment or the use of suction devices to reduce exposure.</p>\",\"PeriodicalId\":9074,\"journal\":{\"name\":\"Bone & Joint Research\",\"volume\":\"12 10\",\"pages\":\"636-643\"},\"PeriodicalIF\":4.7000,\"publicationDate\":\"2023-10-10\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10562079/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Bone & Joint Research\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1302/2046-3758.1210.BJR-2023-0028.R1\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"CELL & TISSUE ENGINEERING\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Bone & Joint Research","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1302/2046-3758.1210.BJR-2023-0028.R1","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CELL & TISSUE ENGINEERING","Score":null,"Total":0}
Diathermy and bone sawing are high aerosol yield procedures.
Aims: Orthopaedic surgery uses many varied instruments with high-speed, high-impact, thermal energy and sometimes heavy instruments, all of which potentially result in aerosolization of contaminated blood, tissue, and bone, raising concerns for clinicians' health. This study quantifies the aerosol exposure by measuring the number and size distribution of the particles reaching the lead surgeon during key orthopaedic operations.
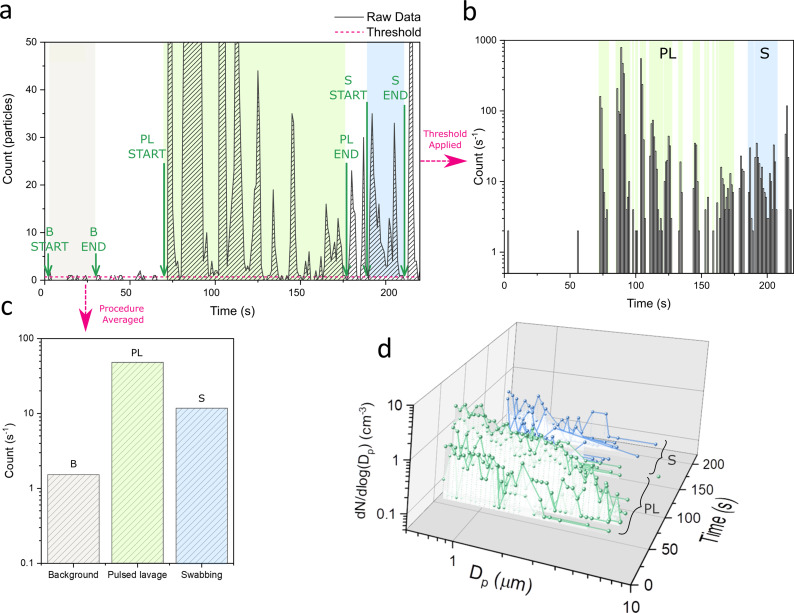
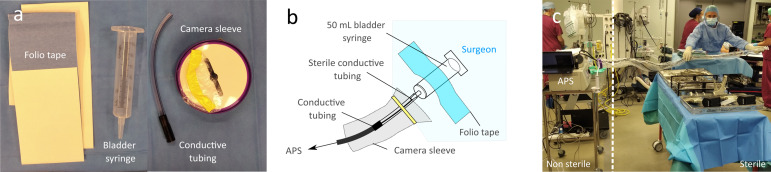
Methods: The aerosol yield from 17 orthopaedic open surgeries (on the knee, hip, and shoulder) was recorded at the position of the lead surgeon using an Aerodynamic Particle Sizer (APS; 0.5 to 20 μm diameter particles) sampling at 1 s time resolution. Through timestamping, detected aerosol was attributed to specific procedures.
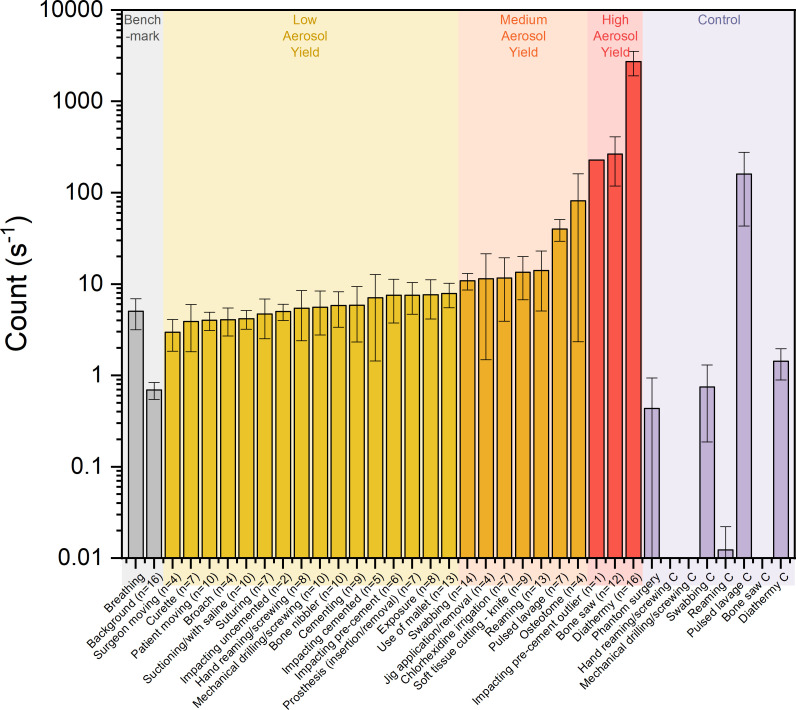
Results: Diathermy (electrocautery) and oscillating bone saw use had a high aerosol yield (> 100 particles detected per s) consistent with high exposure to aerosol in the respirable range (< 5 µm) for the lead surgeon. Pulsed lavage, reaming, osteotome use, and jig application/removal were medium aerosol yield (10 to 100 particles s-1). However, pulsed lavage aerosol was largely attributed to the saline jet, osteotome use was always brief, and jig application/removal had a large variability in the associated aerosol yield. Suctioning (with/without saline irrigation) had a low aerosol yield (< 10 particles s-1). Most surprisingly, other high-speed procedures, such as drilling and screwing, had low aerosol yields.
Conclusion: This work suggests that additional precautions should be recommended for diathermy and bone sawing, such as enhanced personal protective equipment or the use of suction devices to reduce exposure.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
