Afsheen Nasir, Mohammad A Zafar, Mohamed Abdelbaky, Dimitra Papanikolaou, Hesham Ellauzi, Maryam Shaikh, Bulat A Ziganshin, John A Elefteriades
{"title":"降主动脉和胸腹主动脉置换术中脑脊液引流的安全性。","authors":"Afsheen Nasir, Mohammad A Zafar, Mohamed Abdelbaky, Dimitra Papanikolaou, Hesham Ellauzi, Maryam Shaikh, Bulat A Ziganshin, John A Elefteriades","doi":"10.21037/acs-2023-scp-0121","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Spinal cord injury (SCI) remains a significant morbidity of surgical repair of descending thoracic aortic aneurysms (DTAA) and thoracoabdominal aortic aneurysms (TAAA). We present our 17-year experience with cerebrospinal fluid drainage (CSFD) as a protective strategy during open surgical repair of descending and thoracoabdominal aortic disease.</p><p><strong>Methods: </strong>We conducted a retrospective chart review of 132 patients who underwent open surgical repair of DTAA and TAAA and dissections with concurrent use of CSFD for spinal cord protection. Information regarding survival, postoperative course, and complications related to CSFD use were extracted from electronic health records (EHR) and analyzed.</p><p><strong>Results: </strong>Mean patient age was 65.4±13.0 years, and 82 (62.1%) were male. A CSFD was successfully inserted in all patients. The mean hospital length of stay after surgery was 12.2±11.2 days, and in-hospital mortality was 7.6%. Postoperative transient paresis was observed in 5 patients (3.8%), and permanent paraplegia was seen in 4 (3.0%). CSFD related complications were reported in 25 patients (19%). Complications included persistent cerebrospinal fluid (CSF) leakage, blood-tinged CSF (with subdural hematoma reported in 3 patients) and spinal cutaneous fistula in 9 (7%), 14 (11%), and 1 (1%), respectively. Long term survival was 50.9% at 15 years.</p><p><strong>Conclusions: </strong>CSFD is associated with minor complications, without major sequalae. It is a safe practice and likely contributes innocuously to decreased SCI in patients undergoing open repair of DTAA and TAAA.</p>","PeriodicalId":8067,"journal":{"name":"Annals of cardiothoracic surgery","volume":"12 5","pages":"476-483"},"PeriodicalIF":3.1000,"publicationDate":"2023-09-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/87/ee/acs-12-05-476.PMC10561341.pdf","citationCount":"0","resultStr":"{\"title\":\"Safety of cerebrospinal fluid drainage in descending and thoracoabdominal aortic replacement surgery.\",\"authors\":\"Afsheen Nasir, Mohammad A Zafar, Mohamed Abdelbaky, Dimitra Papanikolaou, Hesham Ellauzi, Maryam Shaikh, Bulat A Ziganshin, John A Elefteriades\",\"doi\":\"10.21037/acs-2023-scp-0121\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Spinal cord injury (SCI) remains a significant morbidity of surgical repair of descending thoracic aortic aneurysms (DTAA) and thoracoabdominal aortic aneurysms (TAAA). We present our 17-year experience with cerebrospinal fluid drainage (CSFD) as a protective strategy during open surgical repair of descending and thoracoabdominal aortic disease.</p><p><strong>Methods: </strong>We conducted a retrospective chart review of 132 patients who underwent open surgical repair of DTAA and TAAA and dissections with concurrent use of CSFD for spinal cord protection. Information regarding survival, postoperative course, and complications related to CSFD use were extracted from electronic health records (EHR) and analyzed.</p><p><strong>Results: </strong>Mean patient age was 65.4±13.0 years, and 82 (62.1%) were male. A CSFD was successfully inserted in all patients. The mean hospital length of stay after surgery was 12.2±11.2 days, and in-hospital mortality was 7.6%. Postoperative transient paresis was observed in 5 patients (3.8%), and permanent paraplegia was seen in 4 (3.0%). CSFD related complications were reported in 25 patients (19%). Complications included persistent cerebrospinal fluid (CSF) leakage, blood-tinged CSF (with subdural hematoma reported in 3 patients) and spinal cutaneous fistula in 9 (7%), 14 (11%), and 1 (1%), respectively. Long term survival was 50.9% at 15 years.</p><p><strong>Conclusions: </strong>CSFD is associated with minor complications, without major sequalae. It is a safe practice and likely contributes innocuously to decreased SCI in patients undergoing open repair of DTAA and TAAA.</p>\",\"PeriodicalId\":8067,\"journal\":{\"name\":\"Annals of cardiothoracic surgery\",\"volume\":\"12 5\",\"pages\":\"476-483\"},\"PeriodicalIF\":3.1000,\"publicationDate\":\"2023-09-28\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/87/ee/acs-12-05-476.PMC10561341.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Annals of cardiothoracic surgery\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.21037/acs-2023-scp-0121\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/9/22 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of cardiothoracic surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.21037/acs-2023-scp-0121","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/9/22 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Safety of cerebrospinal fluid drainage in descending and thoracoabdominal aortic replacement surgery.
Background: Spinal cord injury (SCI) remains a significant morbidity of surgical repair of descending thoracic aortic aneurysms (DTAA) and thoracoabdominal aortic aneurysms (TAAA). We present our 17-year experience with cerebrospinal fluid drainage (CSFD) as a protective strategy during open surgical repair of descending and thoracoabdominal aortic disease.
Methods: We conducted a retrospective chart review of 132 patients who underwent open surgical repair of DTAA and TAAA and dissections with concurrent use of CSFD for spinal cord protection. Information regarding survival, postoperative course, and complications related to CSFD use were extracted from electronic health records (EHR) and analyzed.
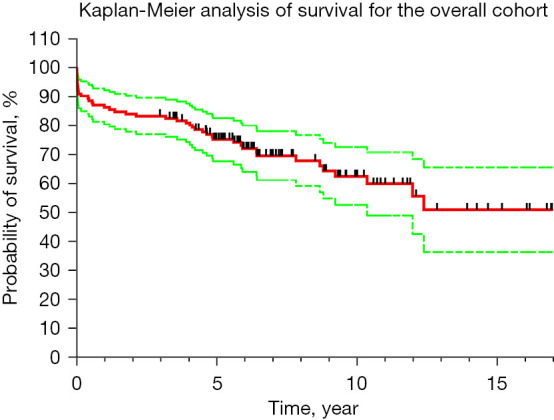
Results: Mean patient age was 65.4±13.0 years, and 82 (62.1%) were male. A CSFD was successfully inserted in all patients. The mean hospital length of stay after surgery was 12.2±11.2 days, and in-hospital mortality was 7.6%. Postoperative transient paresis was observed in 5 patients (3.8%), and permanent paraplegia was seen in 4 (3.0%). CSFD related complications were reported in 25 patients (19%). Complications included persistent cerebrospinal fluid (CSF) leakage, blood-tinged CSF (with subdural hematoma reported in 3 patients) and spinal cutaneous fistula in 9 (7%), 14 (11%), and 1 (1%), respectively. Long term survival was 50.9% at 15 years.
Conclusions: CSFD is associated with minor complications, without major sequalae. It is a safe practice and likely contributes innocuously to decreased SCI in patients undergoing open repair of DTAA and TAAA.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
