{"title":"急诊科新冠肺炎患者氧疗失败的预测因素。","authors":"Karn Suttapanit, Peeraya Lerdpaisarn, Pitsucha Sanguanwit, Praphaphorn Supatanakij","doi":"10.2147/OAEM.S430600","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Most patients with coronavirus disease 2019 (COVID-19) pneumonia require oxygen therapy, including standard oxygen therapy and a high-flow nasal cannula (HFNC), in the Emergency Department (ED), and some patients develop respiratory failure. In the COVID-19 pandemic, the intensive care unit (ICU) was overburdening. Therefore, prioritizing patients who require intensive care is important. This study aimed to find predictors and develop a model to predict patients at risk of requiring an invasive mechanical ventilator (IMV) in the ED.</p><p><strong>Methods: </strong>We performed a retrospective, single-center, observational study. Patients aged ≥18 years who were diagnosed with COVID-19 and required oxygen therapy in the ED were enrolled. Cox regression and Harrell's C-statistic were used to identifying predictors of requiring IMV. The predictive model was developed by calculated coefficients and the ventilator-free survival probability. The predictive model was internally validated using the bootstrapping method.</p><p><strong>Results: </strong>We enrolled 333 patients, and 97 (29.1%) had required IMV. Most 66 (68.0%) failure cases were initial oxygen therapy with HFNC. Respiratory rate-oxygenation (ROX) index, interleukin-6 (IL-6) concentrations ≥20 pg/mL, the SOFA (Sequential Organ Failure Assessment) score without a respiratory score, and the patient's age were independent risk factors of requiring IMV. These factors were used to develop the predictive model. ROX index and the predictive model at 2 hours showed a good performance to predict oxygen therapy failure; the c-statistic was 0.814 (95% confidence level [CI] 0.767-0.861) and 0.901 (95% CI 0.873-0.928), respectively. ROX index ≤5.1 and the predictive model score ≥8 indicated a high probability of requiring IMV.</p><p><strong>Conclusion: </strong>The COVID-19 pandemic was limited resources, ROX index, IL-6 ≥20 pg/mL, the SOFA score without a respiratory score, and the patient's age can be used to predict oxygen therapy failure. Moreover, the predictive model is good at discriminating patients at risk of requiring IMV and close monitoring.</p>","PeriodicalId":45096,"journal":{"name":"Open Access Emergency Medicine","volume":"15 ","pages":"355-365"},"PeriodicalIF":1.5000,"publicationDate":"2023-10-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/b0/8e/oaem-15-355.PMC10560766.pdf","citationCount":"0","resultStr":"{\"title\":\"Predictive Factors of Oxygen Therapy Failure in Patients with COVID-19 in the Emergency Department.\",\"authors\":\"Karn Suttapanit, Peeraya Lerdpaisarn, Pitsucha Sanguanwit, Praphaphorn Supatanakij\",\"doi\":\"10.2147/OAEM.S430600\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Most patients with coronavirus disease 2019 (COVID-19) pneumonia require oxygen therapy, including standard oxygen therapy and a high-flow nasal cannula (HFNC), in the Emergency Department (ED), and some patients develop respiratory failure. In the COVID-19 pandemic, the intensive care unit (ICU) was overburdening. Therefore, prioritizing patients who require intensive care is important. This study aimed to find predictors and develop a model to predict patients at risk of requiring an invasive mechanical ventilator (IMV) in the ED.</p><p><strong>Methods: </strong>We performed a retrospective, single-center, observational study. Patients aged ≥18 years who were diagnosed with COVID-19 and required oxygen therapy in the ED were enrolled. Cox regression and Harrell's C-statistic were used to identifying predictors of requiring IMV. The predictive model was developed by calculated coefficients and the ventilator-free survival probability. The predictive model was internally validated using the bootstrapping method.</p><p><strong>Results: </strong>We enrolled 333 patients, and 97 (29.1%) had required IMV. Most 66 (68.0%) failure cases were initial oxygen therapy with HFNC. Respiratory rate-oxygenation (ROX) index, interleukin-6 (IL-6) concentrations ≥20 pg/mL, the SOFA (Sequential Organ Failure Assessment) score without a respiratory score, and the patient's age were independent risk factors of requiring IMV. These factors were used to develop the predictive model. ROX index and the predictive model at 2 hours showed a good performance to predict oxygen therapy failure; the c-statistic was 0.814 (95% confidence level [CI] 0.767-0.861) and 0.901 (95% CI 0.873-0.928), respectively. ROX index ≤5.1 and the predictive model score ≥8 indicated a high probability of requiring IMV.</p><p><strong>Conclusion: </strong>The COVID-19 pandemic was limited resources, ROX index, IL-6 ≥20 pg/mL, the SOFA score without a respiratory score, and the patient's age can be used to predict oxygen therapy failure. Moreover, the predictive model is good at discriminating patients at risk of requiring IMV and close monitoring.</p>\",\"PeriodicalId\":45096,\"journal\":{\"name\":\"Open Access Emergency Medicine\",\"volume\":\"15 \",\"pages\":\"355-365\"},\"PeriodicalIF\":1.5000,\"publicationDate\":\"2023-10-04\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/b0/8e/oaem-15-355.PMC10560766.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Open Access Emergency Medicine\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.2147/OAEM.S430600\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"EMERGENCY MEDICINE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Open Access Emergency Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/OAEM.S430600","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"EMERGENCY MEDICINE","Score":null,"Total":0}
Predictive Factors of Oxygen Therapy Failure in Patients with COVID-19 in the Emergency Department.
Background: Most patients with coronavirus disease 2019 (COVID-19) pneumonia require oxygen therapy, including standard oxygen therapy and a high-flow nasal cannula (HFNC), in the Emergency Department (ED), and some patients develop respiratory failure. In the COVID-19 pandemic, the intensive care unit (ICU) was overburdening. Therefore, prioritizing patients who require intensive care is important. This study aimed to find predictors and develop a model to predict patients at risk of requiring an invasive mechanical ventilator (IMV) in the ED.
Methods: We performed a retrospective, single-center, observational study. Patients aged ≥18 years who were diagnosed with COVID-19 and required oxygen therapy in the ED were enrolled. Cox regression and Harrell's C-statistic were used to identifying predictors of requiring IMV. The predictive model was developed by calculated coefficients and the ventilator-free survival probability. The predictive model was internally validated using the bootstrapping method.
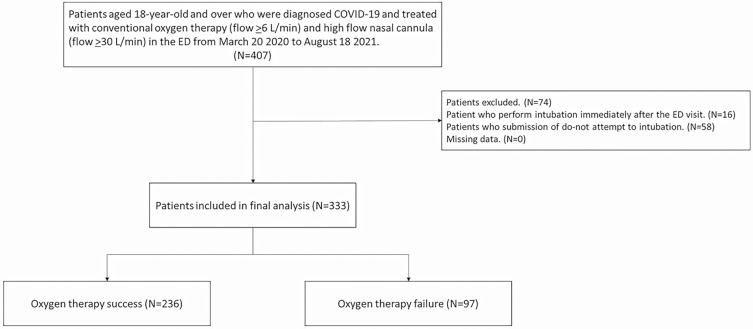
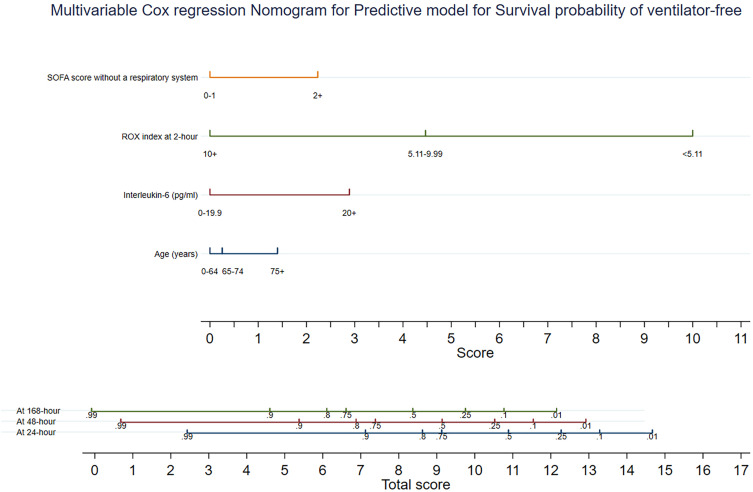
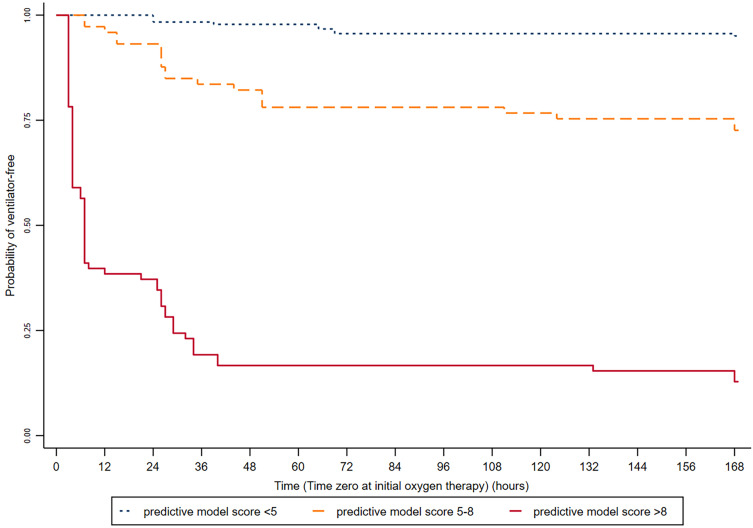
Results: We enrolled 333 patients, and 97 (29.1%) had required IMV. Most 66 (68.0%) failure cases were initial oxygen therapy with HFNC. Respiratory rate-oxygenation (ROX) index, interleukin-6 (IL-6) concentrations ≥20 pg/mL, the SOFA (Sequential Organ Failure Assessment) score without a respiratory score, and the patient's age were independent risk factors of requiring IMV. These factors were used to develop the predictive model. ROX index and the predictive model at 2 hours showed a good performance to predict oxygen therapy failure; the c-statistic was 0.814 (95% confidence level [CI] 0.767-0.861) and 0.901 (95% CI 0.873-0.928), respectively. ROX index ≤5.1 and the predictive model score ≥8 indicated a high probability of requiring IMV.
Conclusion: The COVID-19 pandemic was limited resources, ROX index, IL-6 ≥20 pg/mL, the SOFA score without a respiratory score, and the patient's age can be used to predict oxygen therapy failure. Moreover, the predictive model is good at discriminating patients at risk of requiring IMV and close monitoring.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
