Nikesh Parekh, Khalid Ali, John Graham Davies, Jennifer M Stevenson, Winston Banya, Stephen Nyangoma, Rebekah Schiff, Tischa van der Cammen, Jatinder Harchowal, Chakravarthi Rajkumar
{"title":"老年人出院后的药物相关伤害:预测工具的开发和验证","authors":"Nikesh Parekh, Khalid Ali, John Graham Davies, Jennifer M Stevenson, Winston Banya, Stephen Nyangoma, Rebekah Schiff, Tischa van der Cammen, Jatinder Harchowal, Chakravarthi Rajkumar","doi":"10.1136/bmjqs-2019-009587","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>To develop and validate a tool to predict the risk of an older adult experiencing medication-related harm (MRH) requiring healthcare use following hospital discharge.</p><p><strong>Design, setting, participants: </strong>Multicentre, prospective cohort study recruiting older adults (≥65 years) discharged from five UK teaching hospitals between 2013 and 2015.</p><p><strong>Primary outcome measure: </strong>Participants were followed up for 8 weeks in the community by senior pharmacists to identify MRH (adverse drug reactions, harm from non-adherence, harm from medication error). Three data sources provided MRH and healthcare use information: hospital readmissions, primary care use, participant telephone interview. Candidate variables for prognostic modelling were selected using two systematic reviews, the views of patients with MRH and an expert panel of clinicians. Multivariable logistic regression with backward elimination, based on the Akaike Information Criterion, was used to develop the PRIME tool. The tool was internally validated.</p><p><strong>Results: </strong>1116 out of 1280 recruited participants completed follow-up (87%). Uncertain MRH cases ('possible' and 'probable') were excluded, leaving a tool derivation cohort of 818. 119 (15%) participants experienced 'definite' MRH requiring healthcare use and 699 participants did not. Modelling resulted in a prediction tool with eight variables measured at hospital discharge: age, gender, antiplatelet drug, sodium level, antidiabetic drug, past adverse drug reaction, number of medicines, living alone. The tool's discrimination C-statistic was 0.69 (0.66 after validation) and showed good calibration. Decision curve analysis demonstrated the potential value of the tool to guide clinical decision making compared with alternative approaches.</p><p><strong>Conclusions: </strong>The PRIME tool could be used to identify older patients at high risk of MRH requiring healthcare use following hospital discharge. Prior to clinical use we recommend the tool's evaluation in other settings.</p>","PeriodicalId":49653,"journal":{"name":"Quality & Safety in Health Care","volume":"29 1","pages":"142-153"},"PeriodicalIF":0.0000,"publicationDate":"2020-02-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7045783/pdf/","citationCount":"0","resultStr":"{\"title\":\"Medication-related harm in older adults following hospital discharge: development and validation of a prediction tool.\",\"authors\":\"Nikesh Parekh, Khalid Ali, John Graham Davies, Jennifer M Stevenson, Winston Banya, Stephen Nyangoma, Rebekah Schiff, Tischa van der Cammen, Jatinder Harchowal, Chakravarthi Rajkumar\",\"doi\":\"10.1136/bmjqs-2019-009587\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objectives: </strong>To develop and validate a tool to predict the risk of an older adult experiencing medication-related harm (MRH) requiring healthcare use following hospital discharge.</p><p><strong>Design, setting, participants: </strong>Multicentre, prospective cohort study recruiting older adults (≥65 years) discharged from five UK teaching hospitals between 2013 and 2015.</p><p><strong>Primary outcome measure: </strong>Participants were followed up for 8 weeks in the community by senior pharmacists to identify MRH (adverse drug reactions, harm from non-adherence, harm from medication error). Three data sources provided MRH and healthcare use information: hospital readmissions, primary care use, participant telephone interview. Candidate variables for prognostic modelling were selected using two systematic reviews, the views of patients with MRH and an expert panel of clinicians. Multivariable logistic regression with backward elimination, based on the Akaike Information Criterion, was used to develop the PRIME tool. The tool was internally validated.</p><p><strong>Results: </strong>1116 out of 1280 recruited participants completed follow-up (87%). Uncertain MRH cases ('possible' and 'probable') were excluded, leaving a tool derivation cohort of 818. 119 (15%) participants experienced 'definite' MRH requiring healthcare use and 699 participants did not. Modelling resulted in a prediction tool with eight variables measured at hospital discharge: age, gender, antiplatelet drug, sodium level, antidiabetic drug, past adverse drug reaction, number of medicines, living alone. The tool's discrimination C-statistic was 0.69 (0.66 after validation) and showed good calibration. Decision curve analysis demonstrated the potential value of the tool to guide clinical decision making compared with alternative approaches.</p><p><strong>Conclusions: </strong>The PRIME tool could be used to identify older patients at high risk of MRH requiring healthcare use following hospital discharge. Prior to clinical use we recommend the tool's evaluation in other settings.</p>\",\"PeriodicalId\":49653,\"journal\":{\"name\":\"Quality & Safety in Health Care\",\"volume\":\"29 1\",\"pages\":\"142-153\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2020-02-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7045783/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Quality & Safety in Health Care\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1136/bmjqs-2019-009587\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2019/9/16 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Quality & Safety in Health Care","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1136/bmjqs-2019-009587","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2019/9/16 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
Medication-related harm in older adults following hospital discharge: development and validation of a prediction tool.
Objectives: To develop and validate a tool to predict the risk of an older adult experiencing medication-related harm (MRH) requiring healthcare use following hospital discharge.
Design, setting, participants: Multicentre, prospective cohort study recruiting older adults (≥65 years) discharged from five UK teaching hospitals between 2013 and 2015.
Primary outcome measure: Participants were followed up for 8 weeks in the community by senior pharmacists to identify MRH (adverse drug reactions, harm from non-adherence, harm from medication error). Three data sources provided MRH and healthcare use information: hospital readmissions, primary care use, participant telephone interview. Candidate variables for prognostic modelling were selected using two systematic reviews, the views of patients with MRH and an expert panel of clinicians. Multivariable logistic regression with backward elimination, based on the Akaike Information Criterion, was used to develop the PRIME tool. The tool was internally validated.
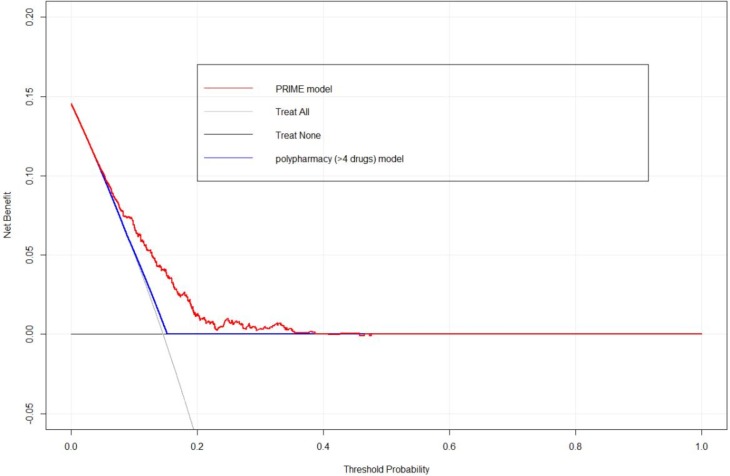
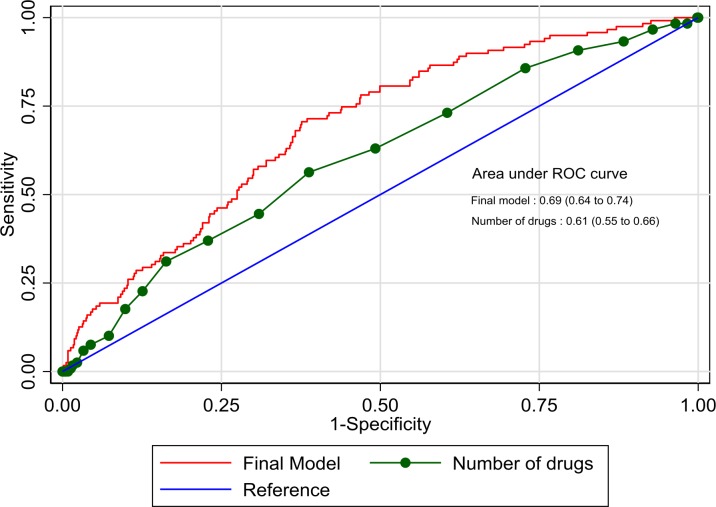
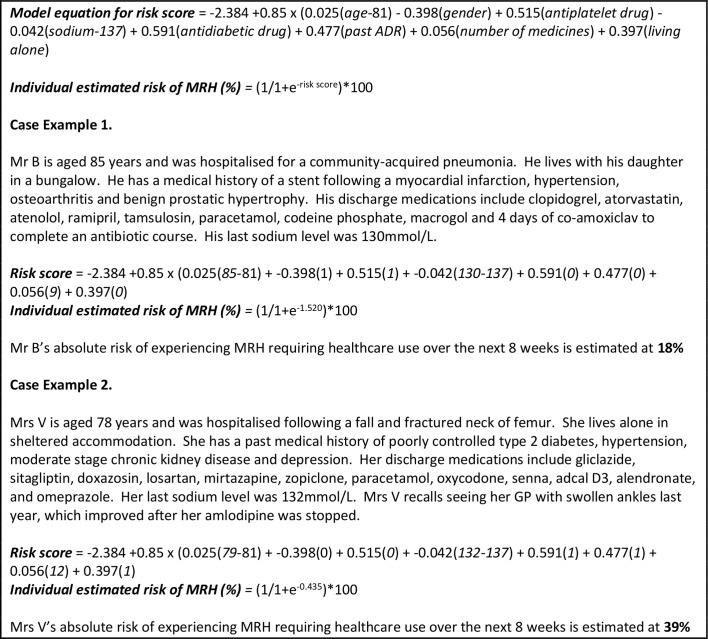
Results: 1116 out of 1280 recruited participants completed follow-up (87%). Uncertain MRH cases ('possible' and 'probable') were excluded, leaving a tool derivation cohort of 818. 119 (15%) participants experienced 'definite' MRH requiring healthcare use and 699 participants did not. Modelling resulted in a prediction tool with eight variables measured at hospital discharge: age, gender, antiplatelet drug, sodium level, antidiabetic drug, past adverse drug reaction, number of medicines, living alone. The tool's discrimination C-statistic was 0.69 (0.66 after validation) and showed good calibration. Decision curve analysis demonstrated the potential value of the tool to guide clinical decision making compared with alternative approaches.
Conclusions: The PRIME tool could be used to identify older patients at high risk of MRH requiring healthcare use following hospital discharge. Prior to clinical use we recommend the tool's evaluation in other settings.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
