{"title":"A型,B型和非萎缩性胃炎","authors":"Sun-Young Lee","doi":"10.7704/kjhugr.2023.0015","DOIUrl":null,"url":null,"abstract":"<p><p>The gastric cancer risk varies based on the etiology and severity of gastritis, which depends on a history of <i>Helicobacter pylori</i> infection and the secretory capacity of the stomach. Type A gastritis is associated with reverse atrophy of the corpus and type B with progressive atrophy extending from the antrum to the corpus. Diffuse or spotty redness in the corpus together with high serum pepsinogen (PG) II levels and a low PG I/II ratio are observed in patients with <i>H. pylori</i> infection when secretory capacity of the stomach is intact. Diffuse-type gastric cancer may develop near the gastric folds, which is a rare site of atrophy. Low serum PG I levels are associated with progressive gastric corpus atrophy and intestinal metaplasia in patients with chronic and previous <i>H. pylori</i> infections. This clinical scenario predisposes patients to intestinal-type gastric cancer, which originates in the atrophic and metaplastic gastric mucosa. Conversely, a high PG I/II ratio is observed in patients without <i>H. pylori</i> infection. Serum PG I levels and the PG I/II ratio are high in patients with acute <i>H. pylori</i>-negative gastritis, including drug-induced gastritis but are significantly low in autoimmune gastritis. Gastric neuroendocrine tumors may develop in patients with autoimmune gastritis or in those with long-term acid suppressant use. Fasting serum gastrin levels and the risk of neuroendocrine tumors are high in both cases. In this review, types of gastritis are summarized along with evaluation performed to determine the secretory capacity of the background gastric mucosa.</p>","PeriodicalId":22895,"journal":{"name":"The Korean Journal of Helicobacter and Upper Gastrointestinal Research","volume":" ","pages":"108-117"},"PeriodicalIF":0.0000,"publicationDate":"2023-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11967552/pdf/","citationCount":"0","resultStr":"{\"title\":\"[Type A, Type B, and Non-atrophic Gastritis].\",\"authors\":\"Sun-Young Lee\",\"doi\":\"10.7704/kjhugr.2023.0015\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>The gastric cancer risk varies based on the etiology and severity of gastritis, which depends on a history of <i>Helicobacter pylori</i> infection and the secretory capacity of the stomach. Type A gastritis is associated with reverse atrophy of the corpus and type B with progressive atrophy extending from the antrum to the corpus. Diffuse or spotty redness in the corpus together with high serum pepsinogen (PG) II levels and a low PG I/II ratio are observed in patients with <i>H. pylori</i> infection when secretory capacity of the stomach is intact. Diffuse-type gastric cancer may develop near the gastric folds, which is a rare site of atrophy. Low serum PG I levels are associated with progressive gastric corpus atrophy and intestinal metaplasia in patients with chronic and previous <i>H. pylori</i> infections. This clinical scenario predisposes patients to intestinal-type gastric cancer, which originates in the atrophic and metaplastic gastric mucosa. Conversely, a high PG I/II ratio is observed in patients without <i>H. pylori</i> infection. Serum PG I levels and the PG I/II ratio are high in patients with acute <i>H. pylori</i>-negative gastritis, including drug-induced gastritis but are significantly low in autoimmune gastritis. Gastric neuroendocrine tumors may develop in patients with autoimmune gastritis or in those with long-term acid suppressant use. Fasting serum gastrin levels and the risk of neuroendocrine tumors are high in both cases. In this review, types of gastritis are summarized along with evaluation performed to determine the secretory capacity of the background gastric mucosa.</p>\",\"PeriodicalId\":22895,\"journal\":{\"name\":\"The Korean Journal of Helicobacter and Upper Gastrointestinal Research\",\"volume\":\" \",\"pages\":\"108-117\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-06-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11967552/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"The Korean Journal of Helicobacter and Upper Gastrointestinal Research\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.7704/kjhugr.2023.0015\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/6/12 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"The Korean Journal of Helicobacter and Upper Gastrointestinal Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.7704/kjhugr.2023.0015","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/6/12 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
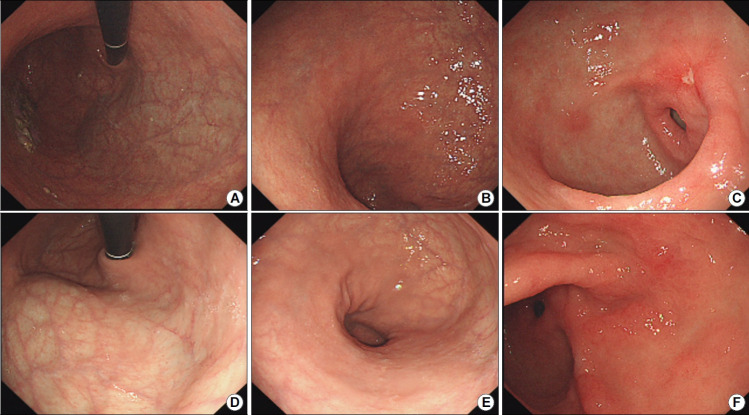
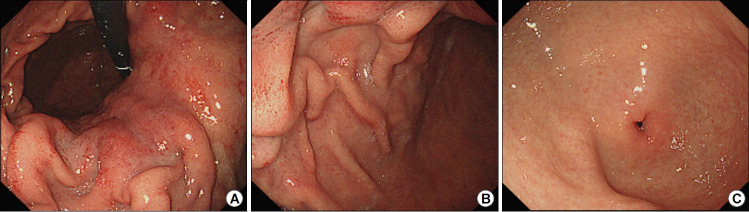
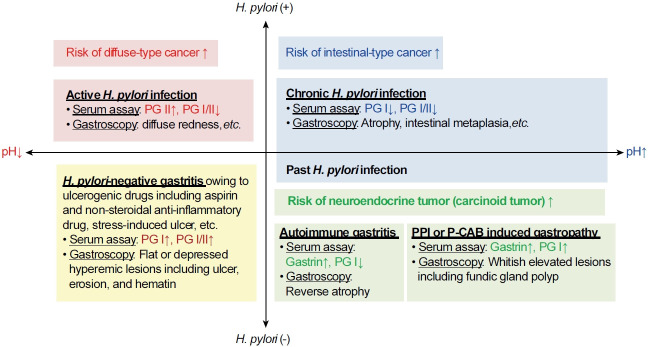
The gastric cancer risk varies based on the etiology and severity of gastritis, which depends on a history of Helicobacter pylori infection and the secretory capacity of the stomach. Type A gastritis is associated with reverse atrophy of the corpus and type B with progressive atrophy extending from the antrum to the corpus. Diffuse or spotty redness in the corpus together with high serum pepsinogen (PG) II levels and a low PG I/II ratio are observed in patients with H. pylori infection when secretory capacity of the stomach is intact. Diffuse-type gastric cancer may develop near the gastric folds, which is a rare site of atrophy. Low serum PG I levels are associated with progressive gastric corpus atrophy and intestinal metaplasia in patients with chronic and previous H. pylori infections. This clinical scenario predisposes patients to intestinal-type gastric cancer, which originates in the atrophic and metaplastic gastric mucosa. Conversely, a high PG I/II ratio is observed in patients without H. pylori infection. Serum PG I levels and the PG I/II ratio are high in patients with acute H. pylori-negative gastritis, including drug-induced gastritis but are significantly low in autoimmune gastritis. Gastric neuroendocrine tumors may develop in patients with autoimmune gastritis or in those with long-term acid suppressant use. Fasting serum gastrin levels and the risk of neuroendocrine tumors are high in both cases. In this review, types of gastritis are summarized along with evaluation performed to determine the secretory capacity of the background gastric mucosa.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
