Rachel Ann Elliott, Matthew J Boyd, Lukasz Tanajewski, Nick Barber, Georgios Gkountouras, Anthony J Avery, Rajnikant Mehta, James E Davies, Nde-Eshimuni Salema, Christopher Craig, Asam Latif, Justin Waring, Antony Chuter
{"title":"“新药服务”:支持长期患者开始服用新药的依从性:一项实用随机对照试验的26周随访","authors":"Rachel Ann Elliott, Matthew J Boyd, Lukasz Tanajewski, Nick Barber, Georgios Gkountouras, Anthony J Avery, Rajnikant Mehta, James E Davies, Nde-Eshimuni Salema, Christopher Craig, Asam Latif, Justin Waring, Antony Chuter","doi":"10.1136/bmjqs-2018-009177","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>To examine the effectiveness and cost-effectiveness of the community pharmacy New Medicine Service (NMS) at 26 weeks.</p><p><strong>Methods: </strong>Pragmatic patient-level parallel randomised controlled trial in 46 English community pharmacies. 504 participants aged ≥14, identified in the pharmacy when presenting a prescription for a new medicine for predefined long-term conditions, randomised to receive NMS (n=251) or normal practice (n=253) (NMS intervention: 2 consultations 1 and 2 weeks after prescription presentation). Adherence assessed through patient self-report at 26-week follow-up. Intention-to-treat analysis employed. National Health Service (NHS) costs calculated. Disease-specific Markov models estimating impact of non-adherence combined with clinical trial data to calculate costs per extra quality-adjusted life-year (QALY; NHS England perspective).</p><p><strong>Results: </strong>Unadjusted analysis: of 327 patients still taking the initial medicine, 97/170 (57.1%) and 103/157 (65.6%) (p=0.113) patients were adherent in normal practice and NMS arms, respectively. Adjusted intention-to-treat analysis: adherence OR 1.50 (95% CI 0.93 to 2.44, p=0.095), in favour of NMS. There was a non-significant reduction in 26-week NHS costs for NMS: -£104 (95% CI -£37 to £257, p=0.168) per patient. NMS generated a mean of 0.04 (95% CI -0.01 to 0.13) more QALYs per patient, with mean reduction in lifetime cost of -£113.9 (-1159.4, 683.7). The incremental cost-effectiveness ratio was -£2758/QALY (2.5% and 97.5%: -38 739.5, 34 024.2. NMS has an 89% probability of cost-effectiveness at a willingness to pay of £20 000 per QALY.</p><p><strong>Conclusions: </strong>At 26-week follow-up, NMS was unable to demonstrate a statistically significant increase in adherence or reduction in NHS costs, which may be attributable to patient attrition from the study. Long-term economic evaluation suggested NMS may deliver better patient outcomes and reduced overall healthcare costs than normal practice, but uncertainty around this finding is high.</p><p><strong>Trial registration number: </strong>NCT01635361, ISRCTN23560818, ISRCTN23560818, UKCRN12494.</p>","PeriodicalId":49653,"journal":{"name":"Quality & Safety in Health Care","volume":"29 1","pages":"286-295"},"PeriodicalIF":0.0000,"publicationDate":"2020-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7146933/pdf/","citationCount":"0","resultStr":"{\"title\":\"'New Medicine Service': supporting adherence in people starting a new medication for a long-term condition: 26-week follow-up of a pragmatic randomised controlled trial.\",\"authors\":\"Rachel Ann Elliott, Matthew J Boyd, Lukasz Tanajewski, Nick Barber, Georgios Gkountouras, Anthony J Avery, Rajnikant Mehta, James E Davies, Nde-Eshimuni Salema, Christopher Craig, Asam Latif, Justin Waring, Antony Chuter\",\"doi\":\"10.1136/bmjqs-2018-009177\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>To examine the effectiveness and cost-effectiveness of the community pharmacy New Medicine Service (NMS) at 26 weeks.</p><p><strong>Methods: </strong>Pragmatic patient-level parallel randomised controlled trial in 46 English community pharmacies. 504 participants aged ≥14, identified in the pharmacy when presenting a prescription for a new medicine for predefined long-term conditions, randomised to receive NMS (n=251) or normal practice (n=253) (NMS intervention: 2 consultations 1 and 2 weeks after prescription presentation). Adherence assessed through patient self-report at 26-week follow-up. Intention-to-treat analysis employed. National Health Service (NHS) costs calculated. Disease-specific Markov models estimating impact of non-adherence combined with clinical trial data to calculate costs per extra quality-adjusted life-year (QALY; NHS England perspective).</p><p><strong>Results: </strong>Unadjusted analysis: of 327 patients still taking the initial medicine, 97/170 (57.1%) and 103/157 (65.6%) (p=0.113) patients were adherent in normal practice and NMS arms, respectively. Adjusted intention-to-treat analysis: adherence OR 1.50 (95% CI 0.93 to 2.44, p=0.095), in favour of NMS. There was a non-significant reduction in 26-week NHS costs for NMS: -£104 (95% CI -£37 to £257, p=0.168) per patient. NMS generated a mean of 0.04 (95% CI -0.01 to 0.13) more QALYs per patient, with mean reduction in lifetime cost of -£113.9 (-1159.4, 683.7). The incremental cost-effectiveness ratio was -£2758/QALY (2.5% and 97.5%: -38 739.5, 34 024.2. NMS has an 89% probability of cost-effectiveness at a willingness to pay of £20 000 per QALY.</p><p><strong>Conclusions: </strong>At 26-week follow-up, NMS was unable to demonstrate a statistically significant increase in adherence or reduction in NHS costs, which may be attributable to patient attrition from the study. Long-term economic evaluation suggested NMS may deliver better patient outcomes and reduced overall healthcare costs than normal practice, but uncertainty around this finding is high.</p><p><strong>Trial registration number: </strong>NCT01635361, ISRCTN23560818, ISRCTN23560818, UKCRN12494.</p>\",\"PeriodicalId\":49653,\"journal\":{\"name\":\"Quality & Safety in Health Care\",\"volume\":\"29 1\",\"pages\":\"286-295\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2020-04-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7146933/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Quality & Safety in Health Care\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1136/bmjqs-2018-009177\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2019/11/15 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Quality & Safety in Health Care","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1136/bmjqs-2018-009177","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2019/11/15 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
'New Medicine Service': supporting adherence in people starting a new medication for a long-term condition: 26-week follow-up of a pragmatic randomised controlled trial.
Objective: To examine the effectiveness and cost-effectiveness of the community pharmacy New Medicine Service (NMS) at 26 weeks.
Methods: Pragmatic patient-level parallel randomised controlled trial in 46 English community pharmacies. 504 participants aged ≥14, identified in the pharmacy when presenting a prescription for a new medicine for predefined long-term conditions, randomised to receive NMS (n=251) or normal practice (n=253) (NMS intervention: 2 consultations 1 and 2 weeks after prescription presentation). Adherence assessed through patient self-report at 26-week follow-up. Intention-to-treat analysis employed. National Health Service (NHS) costs calculated. Disease-specific Markov models estimating impact of non-adherence combined with clinical trial data to calculate costs per extra quality-adjusted life-year (QALY; NHS England perspective).
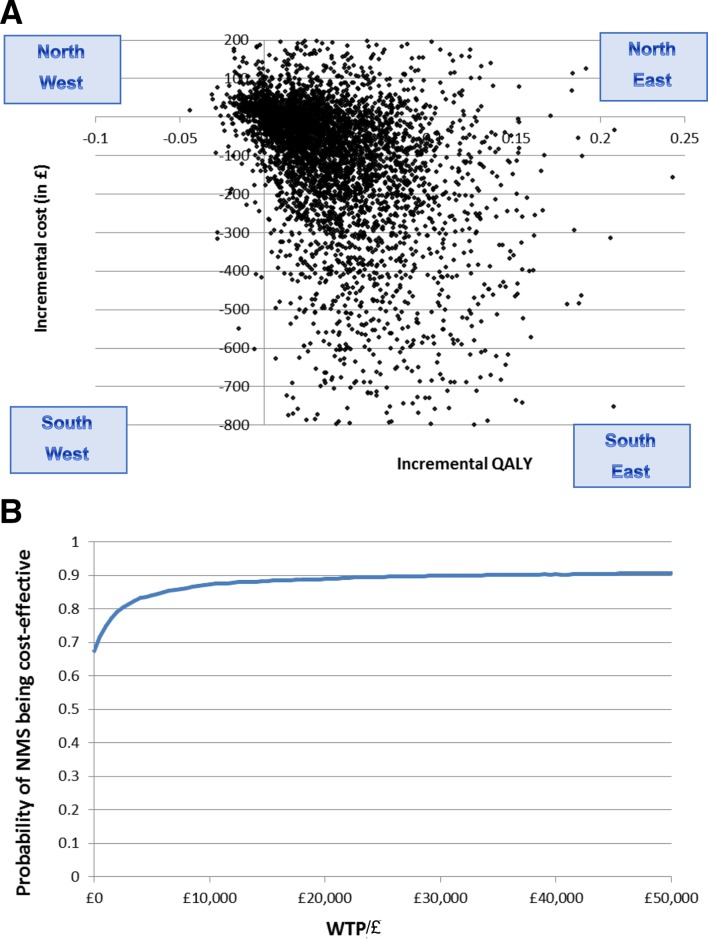
Results: Unadjusted analysis: of 327 patients still taking the initial medicine, 97/170 (57.1%) and 103/157 (65.6%) (p=0.113) patients were adherent in normal practice and NMS arms, respectively. Adjusted intention-to-treat analysis: adherence OR 1.50 (95% CI 0.93 to 2.44, p=0.095), in favour of NMS. There was a non-significant reduction in 26-week NHS costs for NMS: -£104 (95% CI -£37 to £257, p=0.168) per patient. NMS generated a mean of 0.04 (95% CI -0.01 to 0.13) more QALYs per patient, with mean reduction in lifetime cost of -£113.9 (-1159.4, 683.7). The incremental cost-effectiveness ratio was -£2758/QALY (2.5% and 97.5%: -38 739.5, 34 024.2. NMS has an 89% probability of cost-effectiveness at a willingness to pay of £20 000 per QALY.
Conclusions: At 26-week follow-up, NMS was unable to demonstrate a statistically significant increase in adherence or reduction in NHS costs, which may be attributable to patient attrition from the study. Long-term economic evaluation suggested NMS may deliver better patient outcomes and reduced overall healthcare costs than normal practice, but uncertainty around this finding is high.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
