Alain K Koyama, Claire-Sophie Sheridan Maddox, Ling Li, Tracey Bucknall, Johanna I Westbrook
{"title":"双重检查减少药物管理错误的有效性:系统回顾","authors":"Alain K Koyama, Claire-Sophie Sheridan Maddox, Ling Li, Tracey Bucknall, Johanna I Westbrook","doi":"10.1136/bmjqs-2019-009552","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Double checking medication administration in hospitals is often standard practice, particularly for high-risk drugs, yet its effectiveness in reducing medication administration errors (MAEs) and improving patient outcomes remains unclear. We conducted a systematic review of studies evaluating evidence of the effectiveness of double checking to reduce MAEs.</p><p><strong>Methods: </strong>Five databases (PubMed, Embase, CINAHL, Ovid@Journals, OpenGrey) were searched for studies evaluating the use and effectiveness of double checking on reducing medication administration errors in a hospital setting. Included studies were required to report any of three outcome measures: an effect estimate such as a risk ratio or risk difference representing the association between double checking and MAEs, or between double checking and patient harm; or a rate representing adherence to the hospital's double checking policy.</p><p><strong>Results: </strong>Thirteen studies were identified, including 10 studies using an observational study design, two randomised controlled trials and one randomised trial in a simulated setting. Studies included both paediatric and adult inpatient populations and varied considerably in quality. Among three good quality studies, only one showed a significant association between double checking and a reduction in MAEs, another showed no association, and the third study reported only adherence rates. No studies investigated changes in medication-related harm associated with double checking. Reported double checking adherence rates ranged from 52% to 97% of administrations. Only three studies reported if and how independent and primed double checking were differentiated.</p><p><strong>Conclusion: </strong>There is insufficient evidence that double versus single checking of medication administration is associated with lower rates of MAEs or reduced harm. Most comparative studies fail to define or investigate the level of adherence to independent double checking, further limiting conclusions regarding effectiveness in error prevention. Higher-quality studies are needed to determine if, and in what context (eg, drug type, setting), double checking produces sufficient benefits in patient safety to warrant the considerable resources required. CRD42018103436.</p>","PeriodicalId":49653,"journal":{"name":"Quality & Safety in Health Care","volume":"29 1","pages":"595-603"},"PeriodicalIF":0.0000,"publicationDate":"2020-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7362775/pdf/","citationCount":"0","resultStr":"{\"title\":\"Effectiveness of double checking to reduce medication administration errors: a systematic review.\",\"authors\":\"Alain K Koyama, Claire-Sophie Sheridan Maddox, Ling Li, Tracey Bucknall, Johanna I Westbrook\",\"doi\":\"10.1136/bmjqs-2019-009552\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Double checking medication administration in hospitals is often standard practice, particularly for high-risk drugs, yet its effectiveness in reducing medication administration errors (MAEs) and improving patient outcomes remains unclear. We conducted a systematic review of studies evaluating evidence of the effectiveness of double checking to reduce MAEs.</p><p><strong>Methods: </strong>Five databases (PubMed, Embase, CINAHL, Ovid@Journals, OpenGrey) were searched for studies evaluating the use and effectiveness of double checking on reducing medication administration errors in a hospital setting. Included studies were required to report any of three outcome measures: an effect estimate such as a risk ratio or risk difference representing the association between double checking and MAEs, or between double checking and patient harm; or a rate representing adherence to the hospital's double checking policy.</p><p><strong>Results: </strong>Thirteen studies were identified, including 10 studies using an observational study design, two randomised controlled trials and one randomised trial in a simulated setting. Studies included both paediatric and adult inpatient populations and varied considerably in quality. Among three good quality studies, only one showed a significant association between double checking and a reduction in MAEs, another showed no association, and the third study reported only adherence rates. No studies investigated changes in medication-related harm associated with double checking. Reported double checking adherence rates ranged from 52% to 97% of administrations. Only three studies reported if and how independent and primed double checking were differentiated.</p><p><strong>Conclusion: </strong>There is insufficient evidence that double versus single checking of medication administration is associated with lower rates of MAEs or reduced harm. Most comparative studies fail to define or investigate the level of adherence to independent double checking, further limiting conclusions regarding effectiveness in error prevention. Higher-quality studies are needed to determine if, and in what context (eg, drug type, setting), double checking produces sufficient benefits in patient safety to warrant the considerable resources required. CRD42018103436.</p>\",\"PeriodicalId\":49653,\"journal\":{\"name\":\"Quality & Safety in Health Care\",\"volume\":\"29 1\",\"pages\":\"595-603\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2020-07-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7362775/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Quality & Safety in Health Care\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1136/bmjqs-2019-009552\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2019/8/7 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Quality & Safety in Health Care","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1136/bmjqs-2019-009552","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2019/8/7 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
Effectiveness of double checking to reduce medication administration errors: a systematic review.
Background: Double checking medication administration in hospitals is often standard practice, particularly for high-risk drugs, yet its effectiveness in reducing medication administration errors (MAEs) and improving patient outcomes remains unclear. We conducted a systematic review of studies evaluating evidence of the effectiveness of double checking to reduce MAEs.
Methods: Five databases (PubMed, Embase, CINAHL, Ovid@Journals, OpenGrey) were searched for studies evaluating the use and effectiveness of double checking on reducing medication administration errors in a hospital setting. Included studies were required to report any of three outcome measures: an effect estimate such as a risk ratio or risk difference representing the association between double checking and MAEs, or between double checking and patient harm; or a rate representing adherence to the hospital's double checking policy.
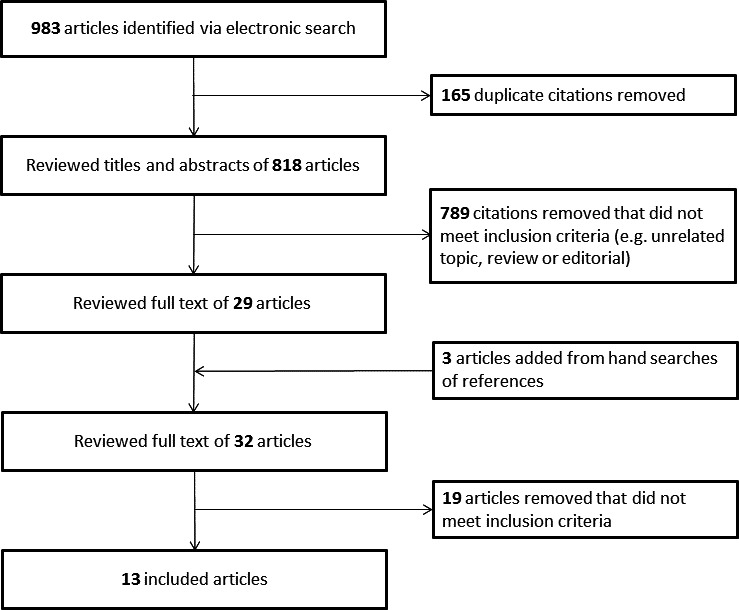
Results: Thirteen studies were identified, including 10 studies using an observational study design, two randomised controlled trials and one randomised trial in a simulated setting. Studies included both paediatric and adult inpatient populations and varied considerably in quality. Among three good quality studies, only one showed a significant association between double checking and a reduction in MAEs, another showed no association, and the third study reported only adherence rates. No studies investigated changes in medication-related harm associated with double checking. Reported double checking adherence rates ranged from 52% to 97% of administrations. Only three studies reported if and how independent and primed double checking were differentiated.
Conclusion: There is insufficient evidence that double versus single checking of medication administration is associated with lower rates of MAEs or reduced harm. Most comparative studies fail to define or investigate the level of adherence to independent double checking, further limiting conclusions regarding effectiveness in error prevention. Higher-quality studies are needed to determine if, and in what context (eg, drug type, setting), double checking produces sufficient benefits in patient safety to warrant the considerable resources required. CRD42018103436.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
