Leilei Yuan, Mengyan Zhang, Li Xu, Xin Wang, Qian Chen, Lin Ai
{"title":"脊索瘤样脑膜瘤的11C-MET PET和18F-FDG PET特征","authors":"Leilei Yuan, Mengyan Zhang, Li Xu, Xin Wang, Qian Chen, Lin Ai","doi":"10.1002/ird3.6","DOIUrl":null,"url":null,"abstract":"<p>A 17-year-old female patient presented to the neurology department with a 3-month history of left limb numbness and spasm with transient loss of consciousness 3 weeks earlier. A brain MRI revealed a right temporal lobe mass (Figure 1a, arrow) with hypointensity on T1WI, hyperintensity on T2WI, and no diffusion restriction on DWI and ADC mapping. The lesion showed minimal tracer uptake on <sup>18</sup>F-FDG PET (Figure 1b, solid arrowhead) but avid uptake on <sup>11</sup>C-MET PET with an SUVmax of 5.7 (Figure 1c, hollow arrowhead) with the contralateral normal tissue as a reference, suggesting a benign tumor other than inflammatory granuloma or malignant tumor. After conservative treatment with hormone and antiepileptic drugs, the patient's symptoms significantly improved. At the 3-month follow-up, the patient presented again with seizures of the left upper limb and transient loss of consciousness. She underwent mass excision in the neurosurgery department. Histopathology (Figure 1d) revealed a neoplasm with cords or trabeculae of small epithelioid to vacuolated cells embedded in a mucin-rich matrix, characteristic of chordoid meningioma (WHO grade 2), a rare type of meningioma [<span>1-3</span>. Immunostaining for SSTR-2 (Figure 1e), EMA, and PR showed strong reactivity in the tumor cells, and the MIB-1 labeling index was about 1%. Postoperative recovery was good, and no positive symptoms were found during a 5-year follow-up period [<span>4</span>]. This case report highlights the need to consider intracranial chordoid meningioma as a differential diagnosis when there is a discrepancy in the extent of tracer uptake on <sup>11</sup>C-MET and <sup>18</sup>F-FDG PET [<span>5, 6</span>].</p><p><b>Leilei Yuan</b>: Writing – original draft (Lead). <b>Mengyan Zhang</b>: Writing – original draft (Equal). <b>Li Xu</b>: Resources (Supporting). <b>Xin Wang</b>: Writing – original draft (Supporting). <b>Qian Chen</b>: Writing – review & editing (Supporting). <b>Lin Ai</b>: Writing – review & editing (Lead).</p><p>The authors declare no conflicts of interest.</p><p>None.</p><p>None.</p>","PeriodicalId":73508,"journal":{"name":"iRadiology","volume":"1 1","pages":"101-102"},"PeriodicalIF":0.0000,"publicationDate":"2023-03-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/ird3.6","citationCount":"0","resultStr":"{\"title\":\"11C-MET PET and 18F-FDG PET characteristics of chordoid meningioma\",\"authors\":\"Leilei Yuan, Mengyan Zhang, Li Xu, Xin Wang, Qian Chen, Lin Ai\",\"doi\":\"10.1002/ird3.6\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>A 17-year-old female patient presented to the neurology department with a 3-month history of left limb numbness and spasm with transient loss of consciousness 3 weeks earlier. A brain MRI revealed a right temporal lobe mass (Figure 1a, arrow) with hypointensity on T1WI, hyperintensity on T2WI, and no diffusion restriction on DWI and ADC mapping. The lesion showed minimal tracer uptake on <sup>18</sup>F-FDG PET (Figure 1b, solid arrowhead) but avid uptake on <sup>11</sup>C-MET PET with an SUVmax of 5.7 (Figure 1c, hollow arrowhead) with the contralateral normal tissue as a reference, suggesting a benign tumor other than inflammatory granuloma or malignant tumor. After conservative treatment with hormone and antiepileptic drugs, the patient's symptoms significantly improved. At the 3-month follow-up, the patient presented again with seizures of the left upper limb and transient loss of consciousness. She underwent mass excision in the neurosurgery department. Histopathology (Figure 1d) revealed a neoplasm with cords or trabeculae of small epithelioid to vacuolated cells embedded in a mucin-rich matrix, characteristic of chordoid meningioma (WHO grade 2), a rare type of meningioma [<span>1-3</span>. Immunostaining for SSTR-2 (Figure 1e), EMA, and PR showed strong reactivity in the tumor cells, and the MIB-1 labeling index was about 1%. Postoperative recovery was good, and no positive symptoms were found during a 5-year follow-up period [<span>4</span>]. This case report highlights the need to consider intracranial chordoid meningioma as a differential diagnosis when there is a discrepancy in the extent of tracer uptake on <sup>11</sup>C-MET and <sup>18</sup>F-FDG PET [<span>5, 6</span>].</p><p><b>Leilei Yuan</b>: Writing – original draft (Lead). <b>Mengyan Zhang</b>: Writing – original draft (Equal). <b>Li Xu</b>: Resources (Supporting). <b>Xin Wang</b>: Writing – original draft (Supporting). <b>Qian Chen</b>: Writing – review & editing (Supporting). <b>Lin Ai</b>: Writing – review & editing (Lead).</p><p>The authors declare no conflicts of interest.</p><p>None.</p><p>None.</p>\",\"PeriodicalId\":73508,\"journal\":{\"name\":\"iRadiology\",\"volume\":\"1 1\",\"pages\":\"101-102\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-03-19\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/ird3.6\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"iRadiology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/ird3.6\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"iRadiology","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/ird3.6","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
11C-MET PET and 18F-FDG PET characteristics of chordoid meningioma
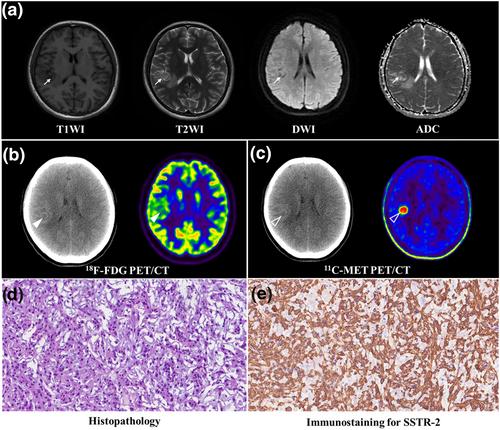
A 17-year-old female patient presented to the neurology department with a 3-month history of left limb numbness and spasm with transient loss of consciousness 3 weeks earlier. A brain MRI revealed a right temporal lobe mass (Figure 1a, arrow) with hypointensity on T1WI, hyperintensity on T2WI, and no diffusion restriction on DWI and ADC mapping. The lesion showed minimal tracer uptake on 18F-FDG PET (Figure 1b, solid arrowhead) but avid uptake on 11C-MET PET with an SUVmax of 5.7 (Figure 1c, hollow arrowhead) with the contralateral normal tissue as a reference, suggesting a benign tumor other than inflammatory granuloma or malignant tumor. After conservative treatment with hormone and antiepileptic drugs, the patient's symptoms significantly improved. At the 3-month follow-up, the patient presented again with seizures of the left upper limb and transient loss of consciousness. She underwent mass excision in the neurosurgery department. Histopathology (Figure 1d) revealed a neoplasm with cords or trabeculae of small epithelioid to vacuolated cells embedded in a mucin-rich matrix, characteristic of chordoid meningioma (WHO grade 2), a rare type of meningioma [1-3. Immunostaining for SSTR-2 (Figure 1e), EMA, and PR showed strong reactivity in the tumor cells, and the MIB-1 labeling index was about 1%. Postoperative recovery was good, and no positive symptoms were found during a 5-year follow-up period [4]. This case report highlights the need to consider intracranial chordoid meningioma as a differential diagnosis when there is a discrepancy in the extent of tracer uptake on 11C-MET and 18F-FDG PET [5, 6].
Leilei Yuan: Writing – original draft (Lead). Mengyan Zhang: Writing – original draft (Equal). Li Xu: Resources (Supporting). Xin Wang: Writing – original draft (Supporting). Qian Chen: Writing – review & editing (Supporting). Lin Ai: Writing – review & editing (Lead).


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
