{"title":"低镁并不是急性心肌梗死硬性事件的重要预测因子","authors":"Cristina Vassalle, Debora Battaglia, Alessandro Vannucci, Kyriazoula Chatzianagnostou, Patrizia Landi, Caterina Arvia, Clara Carpeggiani","doi":"10.1016/j.bbacli.2016.03.003","DOIUrl":null,"url":null,"abstract":"<div><h3>Background</h3><p>Although magnesium (Mg) has recognized cardioprotective properties and hypomagnesemia is common in patients with acute myocardial infarction (AMI), data regarding the role of Mg as prognostic factor for adverse events are scarce, as well as there are conflicting results on the use of Mg as adjuvant therapy in AMI.</p></div><div><h3>Aim</h3><p>To evaluate the role of Mg as predictor for hard events (HE, all cause death, and nonfatal myocardial infarction) in AMI patients.</p></div><div><h3>Design and patients</h3><p>We studied 406 AMI patients (306 males, age: 67<!--> <!-->±<!--> <!-->12<!--> <!-->years, mean<!--> <!-->±<!--> <!-->SD). Patient data were collected from the Institute electronic databank which saves demographic, clinical, instrumental, therapeutical and follow-up data of all patients admitted to our Coronary Unit.</p></div><div><h3>Results</h3><p>During a mean follow-up period of 21<!--> <!-->±<!--> <!-->18<!--> <!-->months, the combined endpoint accounted for 63 HE, 44 (11%) deaths (35 cardiac deaths), 19 (5%) nonfatal MI.</p><p>The multiple regression model identified glycemia as the only independent determinant of Mg in AMI pts. (T value<!--> <!-->=<!--> <!-->−<!--> <!-->2.8, standard coefficient<!--> <!-->=<!--> <!-->−<!--> <!-->0.15, p<!--> <!--><<!--> <!-->0.01). The Kaplan–Meier survival estimates failed to show a significantly worst outcome in patients presenting low Mg (<<!--> <!-->0.783<!--> <!-->mmol/L, 25th percentile). Aging (><!--> <!-->67<!--> <!-->years—50th percentile), and ejection fraction (<<!--> <!-->40%) remained as prognostic factors for HE in the adjusted Cox multivariate proportional hazard model (HR<!--> <!-->=<!--> <!-->2.8, 95% CI<!--> <!-->=<!--> <!-->1.6–5, p<!--> <!--><<!--> <!-->0.001; HR<!--> <!-->=<!--> <!-->3.2, 95% CI<!--> <!-->=<!--> <!-->1.9–5.3 p<!--> <!--><<!--> <!-->0.001, respectively).</p></div><div><h3>Conclusion</h3><p>The present findings do not support a significant role of low Mg as predictor for HE in AMI.</p></div>","PeriodicalId":72344,"journal":{"name":"BBA clinical","volume":"5 ","pages":"Pages 130-133"},"PeriodicalIF":0.0000,"publicationDate":"2016-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1016/j.bbacli.2016.03.003","citationCount":"3","resultStr":"{\"title\":\"Low magnesium is not a significant predictor of hard events in acute myocardial infarction\",\"authors\":\"Cristina Vassalle, Debora Battaglia, Alessandro Vannucci, Kyriazoula Chatzianagnostou, Patrizia Landi, Caterina Arvia, Clara Carpeggiani\",\"doi\":\"10.1016/j.bbacli.2016.03.003\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div><h3>Background</h3><p>Although magnesium (Mg) has recognized cardioprotective properties and hypomagnesemia is common in patients with acute myocardial infarction (AMI), data regarding the role of Mg as prognostic factor for adverse events are scarce, as well as there are conflicting results on the use of Mg as adjuvant therapy in AMI.</p></div><div><h3>Aim</h3><p>To evaluate the role of Mg as predictor for hard events (HE, all cause death, and nonfatal myocardial infarction) in AMI patients.</p></div><div><h3>Design and patients</h3><p>We studied 406 AMI patients (306 males, age: 67<!--> <!-->±<!--> <!-->12<!--> <!-->years, mean<!--> <!-->±<!--> <!-->SD). Patient data were collected from the Institute electronic databank which saves demographic, clinical, instrumental, therapeutical and follow-up data of all patients admitted to our Coronary Unit.</p></div><div><h3>Results</h3><p>During a mean follow-up period of 21<!--> <!-->±<!--> <!-->18<!--> <!-->months, the combined endpoint accounted for 63 HE, 44 (11%) deaths (35 cardiac deaths), 19 (5%) nonfatal MI.</p><p>The multiple regression model identified glycemia as the only independent determinant of Mg in AMI pts. (T value<!--> <!-->=<!--> <!-->−<!--> <!-->2.8, standard coefficient<!--> <!-->=<!--> <!-->−<!--> <!-->0.15, p<!--> <!--><<!--> <!-->0.01). The Kaplan–Meier survival estimates failed to show a significantly worst outcome in patients presenting low Mg (<<!--> <!-->0.783<!--> <!-->mmol/L, 25th percentile). Aging (><!--> <!-->67<!--> <!-->years—50th percentile), and ejection fraction (<<!--> <!-->40%) remained as prognostic factors for HE in the adjusted Cox multivariate proportional hazard model (HR<!--> <!-->=<!--> <!-->2.8, 95% CI<!--> <!-->=<!--> <!-->1.6–5, p<!--> <!--><<!--> <!-->0.001; HR<!--> <!-->=<!--> <!-->3.2, 95% CI<!--> <!-->=<!--> <!-->1.9–5.3 p<!--> <!--><<!--> <!-->0.001, respectively).</p></div><div><h3>Conclusion</h3><p>The present findings do not support a significant role of low Mg as predictor for HE in AMI.</p></div>\",\"PeriodicalId\":72344,\"journal\":{\"name\":\"BBA clinical\",\"volume\":\"5 \",\"pages\":\"Pages 130-133\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2016-06-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1016/j.bbacli.2016.03.003\",\"citationCount\":\"3\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"BBA clinical\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://www.sciencedirect.com/science/article/pii/S2214647416300071\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2016/3/9 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"BBA clinical","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2214647416300071","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2016/3/9 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 3
摘要
虽然镁(Mg)具有公认的心脏保护作用,并且低镁血症在急性心肌梗死(AMI)患者中很常见,但关于镁作为不良事件预后因素的数据很少,而且在AMI中使用镁作为辅助治疗的结果也存在矛盾。目的评价Mg作为AMI患者硬事件(HE、全因死亡和非致死性心肌梗死)预测因子的作用。设计与患者我们研究了406例AMI患者(306例男性,年龄:67±12岁,平均±SD)。患者数据从研究所电子数据库收集,该数据库保存了我们冠状动脉科收治的所有患者的人口统计、临床、仪器、治疗和随访数据。结果在平均21±18个月的随访期间,合并终点占63例HE, 44例(11%)死亡(35例心脏死亡),19例(5%)非致死性mi。多元回归模型确定血糖是AMI患者中Mg的唯一独立决定因素。(T值=−2.8标准系数=−0.15,p & lt;0.01)。Kaplan-Meier生存估计未能显示低Mg (<0.783 mmol/L,第25百分位)。老化(比;67岁—第50百分位)和射血分数(<在调整后的Cox多因素比例风险模型中(HR = 2.8, 95% CI = 1.6-5, p <0.001;HR = 3.2, 95% CI = 1.9-5.3 p <分别为0.001)。结论目前的研究结果不支持低Mg作为AMI中HE的预测因子的重要作用。
Low magnesium is not a significant predictor of hard events in acute myocardial infarction
Background
Although magnesium (Mg) has recognized cardioprotective properties and hypomagnesemia is common in patients with acute myocardial infarction (AMI), data regarding the role of Mg as prognostic factor for adverse events are scarce, as well as there are conflicting results on the use of Mg as adjuvant therapy in AMI.
Aim
To evaluate the role of Mg as predictor for hard events (HE, all cause death, and nonfatal myocardial infarction) in AMI patients.
Design and patients
We studied 406 AMI patients (306 males, age: 67 ± 12 years, mean ± SD). Patient data were collected from the Institute electronic databank which saves demographic, clinical, instrumental, therapeutical and follow-up data of all patients admitted to our Coronary Unit.
Results
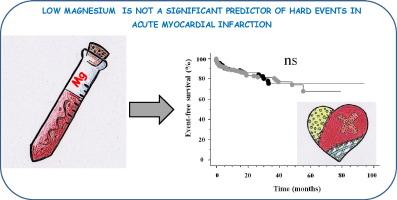
During a mean follow-up period of 21 ± 18 months, the combined endpoint accounted for 63 HE, 44 (11%) deaths (35 cardiac deaths), 19 (5%) nonfatal MI.
The multiple regression model identified glycemia as the only independent determinant of Mg in AMI pts. (T value = − 2.8, standard coefficient = − 0.15, p < 0.01). The Kaplan–Meier survival estimates failed to show a significantly worst outcome in patients presenting low Mg (< 0.783 mmol/L, 25th percentile). Aging (> 67 years—50th percentile), and ejection fraction (< 40%) remained as prognostic factors for HE in the adjusted Cox multivariate proportional hazard model (HR = 2.8, 95% CI = 1.6–5, p < 0.001; HR = 3.2, 95% CI = 1.9–5.3 p < 0.001, respectively).
Conclusion
The present findings do not support a significant role of low Mg as predictor for HE in AMI.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
