Alexander Kc Leung, Benjamin Barankin, Joseph M Lam, Kin Fon Leong
{"title":"儿童喉结型银屑病:最新综述。","authors":"Alexander Kc Leung, Benjamin Barankin, Joseph M Lam, Kin Fon Leong","doi":"10.7573/dic.2023-8-2","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Guttate psoriasis is common and affects 0.5-2% of individuals in the paediatric age group. This review aims to familiarize physicians with the clinical manifestations, evaluation, diagnosis and proper management of guttate psoriasis.</p><p><strong>Methods: </strong>A search was conducted in July 2023 in PubMed Clinical Queries using the key term \"guttate psoriasis\". The search strategy included all observational studies, clinical trials and reviews published within the past 10 years. The information retrieved from the search was used in the compilation of the present article.</p><p><strong>Results: </strong>Guttate psoriasis typically presents with an abrupt onset of numerous, small, scattered, tear-drop-shaped, scaly, erythematous, pruritic papules and plaques. Sites of predilection include the trunk and proximal extremities. There may be a history of preceding streptococcal infection. Koebner phenomenon is characteristic. Guttate psoriasis may spontaneously remit within 3-4 months with no residual scarring, may intermittently recur and, in 40-50% of cases, may persist and progress to chronic plaque psoriasis. Given the possibility for spontaneous remission within several months, active treatment may not be necessary except for cosmetic purposes or because of pruritus. On the other hand, given the high rates of persistence of guttate psoriasis and progression to chronic plaque psoriasis, some authors suggest active treatment of this condition.</p><p><strong>Conclusion: </strong>Various treatment options are available for guttate psoriasis. Triggering and exacerbating factors should be avoided if possible. Topical corticosteroids alone or in combination with other topical agents (e.g. tazarotene and vitamin D analogues) are the most rapid and efficient treatment for guttate psoriasis and are therefore the first-line treatment for mild cases. Other topical therapies include vitamin D analogues, calcineurin inhibitors, anthralin, coal tar and tazarotene. Ultraviolet phototherapy is the first-line therapy for moderate-to-severe guttate psoriasis, as it is more practical than topical therapy when treating widespread or numerous small lesions. Systemic immunosuppressive and immunomodulatory therapies (e.g. methotrexate, cyclosporine, retinoids, fumaric acid esters and biologics) may be considered for patients with moderate-to-severe guttate psoriasis who fail to respond to phototherapy and topical therapies.</p>","PeriodicalId":11362,"journal":{"name":"Drugs in Context","volume":"12 ","pages":""},"PeriodicalIF":2.8000,"publicationDate":"2023-10-23","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10615329/pdf/","citationCount":"0","resultStr":"{\"title\":\"Childhood guttate psoriasis: an updated review.\",\"authors\":\"Alexander Kc Leung, Benjamin Barankin, Joseph M Lam, Kin Fon Leong\",\"doi\":\"10.7573/dic.2023-8-2\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Guttate psoriasis is common and affects 0.5-2% of individuals in the paediatric age group. This review aims to familiarize physicians with the clinical manifestations, evaluation, diagnosis and proper management of guttate psoriasis.</p><p><strong>Methods: </strong>A search was conducted in July 2023 in PubMed Clinical Queries using the key term \\\"guttate psoriasis\\\". The search strategy included all observational studies, clinical trials and reviews published within the past 10 years. The information retrieved from the search was used in the compilation of the present article.</p><p><strong>Results: </strong>Guttate psoriasis typically presents with an abrupt onset of numerous, small, scattered, tear-drop-shaped, scaly, erythematous, pruritic papules and plaques. Sites of predilection include the trunk and proximal extremities. There may be a history of preceding streptococcal infection. Koebner phenomenon is characteristic. Guttate psoriasis may spontaneously remit within 3-4 months with no residual scarring, may intermittently recur and, in 40-50% of cases, may persist and progress to chronic plaque psoriasis. Given the possibility for spontaneous remission within several months, active treatment may not be necessary except for cosmetic purposes or because of pruritus. On the other hand, given the high rates of persistence of guttate psoriasis and progression to chronic plaque psoriasis, some authors suggest active treatment of this condition.</p><p><strong>Conclusion: </strong>Various treatment options are available for guttate psoriasis. Triggering and exacerbating factors should be avoided if possible. Topical corticosteroids alone or in combination with other topical agents (e.g. tazarotene and vitamin D analogues) are the most rapid and efficient treatment for guttate psoriasis and are therefore the first-line treatment for mild cases. Other topical therapies include vitamin D analogues, calcineurin inhibitors, anthralin, coal tar and tazarotene. Ultraviolet phototherapy is the first-line therapy for moderate-to-severe guttate psoriasis, as it is more practical than topical therapy when treating widespread or numerous small lesions. Systemic immunosuppressive and immunomodulatory therapies (e.g. methotrexate, cyclosporine, retinoids, fumaric acid esters and biologics) may be considered for patients with moderate-to-severe guttate psoriasis who fail to respond to phototherapy and topical therapies.</p>\",\"PeriodicalId\":11362,\"journal\":{\"name\":\"Drugs in Context\",\"volume\":\"12 \",\"pages\":\"\"},\"PeriodicalIF\":2.8000,\"publicationDate\":\"2023-10-23\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10615329/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Drugs in Context\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.7573/dic.2023-8-2\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"Pharmacology, Toxicology and Pharmaceutics\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Drugs in Context","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.7573/dic.2023-8-2","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"Pharmacology, Toxicology and Pharmaceutics","Score":null,"Total":0}
Background: Guttate psoriasis is common and affects 0.5-2% of individuals in the paediatric age group. This review aims to familiarize physicians with the clinical manifestations, evaluation, diagnosis and proper management of guttate psoriasis.
Methods: A search was conducted in July 2023 in PubMed Clinical Queries using the key term "guttate psoriasis". The search strategy included all observational studies, clinical trials and reviews published within the past 10 years. The information retrieved from the search was used in the compilation of the present article.
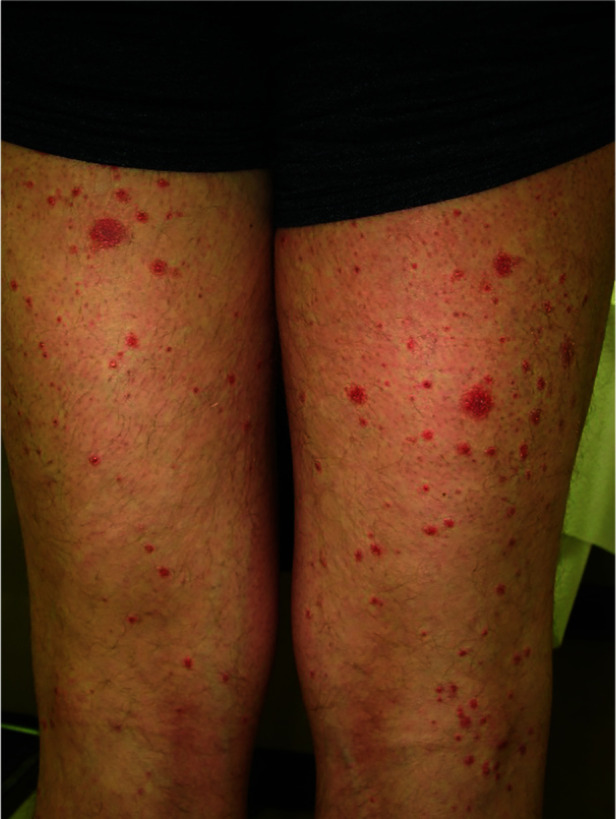
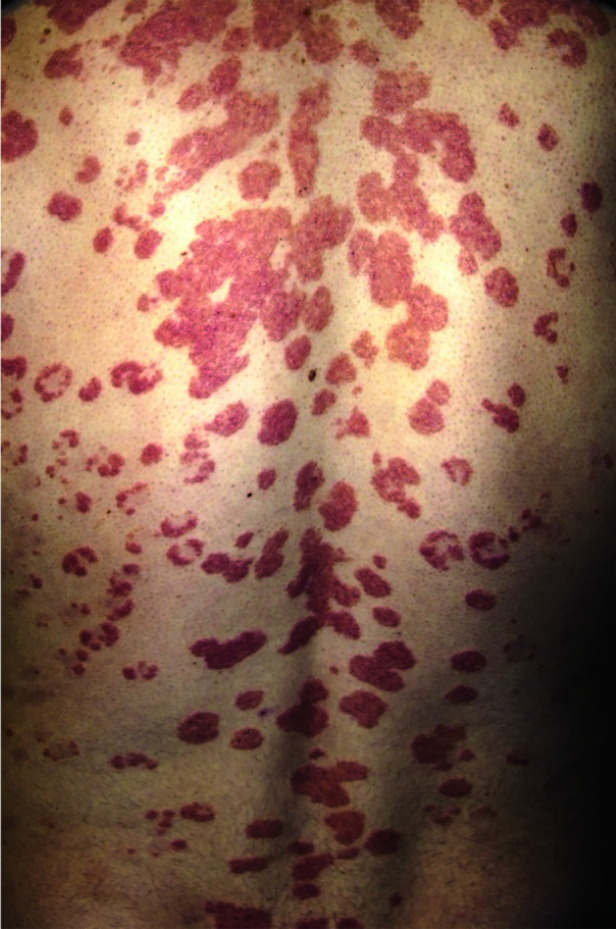
Results: Guttate psoriasis typically presents with an abrupt onset of numerous, small, scattered, tear-drop-shaped, scaly, erythematous, pruritic papules and plaques. Sites of predilection include the trunk and proximal extremities. There may be a history of preceding streptococcal infection. Koebner phenomenon is characteristic. Guttate psoriasis may spontaneously remit within 3-4 months with no residual scarring, may intermittently recur and, in 40-50% of cases, may persist and progress to chronic plaque psoriasis. Given the possibility for spontaneous remission within several months, active treatment may not be necessary except for cosmetic purposes or because of pruritus. On the other hand, given the high rates of persistence of guttate psoriasis and progression to chronic plaque psoriasis, some authors suggest active treatment of this condition.
Conclusion: Various treatment options are available for guttate psoriasis. Triggering and exacerbating factors should be avoided if possible. Topical corticosteroids alone or in combination with other topical agents (e.g. tazarotene and vitamin D analogues) are the most rapid and efficient treatment for guttate psoriasis and are therefore the first-line treatment for mild cases. Other topical therapies include vitamin D analogues, calcineurin inhibitors, anthralin, coal tar and tazarotene. Ultraviolet phototherapy is the first-line therapy for moderate-to-severe guttate psoriasis, as it is more practical than topical therapy when treating widespread or numerous small lesions. Systemic immunosuppressive and immunomodulatory therapies (e.g. methotrexate, cyclosporine, retinoids, fumaric acid esters and biologics) may be considered for patients with moderate-to-severe guttate psoriasis who fail to respond to phototherapy and topical therapies.
期刊介绍:
Covers all phases of original research: laboratory, animal and human/clinical studies, health economics and outcomes research, and postmarketing studies. Original research that shows positive or negative results are welcomed. Invited review articles may cover single-drug reviews, drug class reviews, latest advances in drug therapy, therapeutic-area reviews, place-in-therapy reviews, new pathways and classes of drugs. In addition, systematic reviews and meta-analyses are welcomed and may be published as original research if performed per accepted guidelines. Editorials of key topics and issues in drugs and therapeutics are welcomed. The Editor-in-Chief will also consider manuscripts of interest in areas such as technologies that support diagnosis, assessment and treatment. EQUATOR Network reporting guidelines should be followed for each article type. GPP3 Guidelines should be followed for any industry-sponsored manuscripts. Other Editorial sections may include Editorial, Case Report, Conference Report, Letter-to-the-Editor, Educational Section.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
