Antonella Cotoia, Michele Umbrello, Fiorenza Ferrari, Vincenzo Pota, Francesco Alessandri, Andrea Cortegiani, Silvia De Rosa
{"title":"营养支持和重症监护后综合征的预防:意大利SIAARTI调查。","authors":"Antonella Cotoia, Michele Umbrello, Fiorenza Ferrari, Vincenzo Pota, Francesco Alessandri, Andrea Cortegiani, Silvia De Rosa","doi":"10.1186/s44158-023-00132-4","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Malnutrition and muscle wasting are common in ICU patients and predict adverse patient-centered outcomes. The Italian Society of Anesthesia Analgesia Resuscitation and Intensive Care (SIAARTI) conducted a nationwide survey to identify the nutritional practices in the Italian ICUs and to plan future, training interventions to improve the national clinical practice.</p><p><strong>Methods: </strong>Nationwide online survey, involving Italian ICUs, developed by experts affiliated with SIAARTI. Invitations to participate were distributed through emails and social networks. Data were collected over a period of three months (October 1 to December 31, 2022) during 2022.</p><p><strong>Results: </strong>One hundred full responses from participating ICUs were collected. The number of beds is < 10 in most ICUs and > 20 in 11 ICUs. Most ICUs (87%) are mixed, cardiac (5%), neurosurgical (4%), or pediatric ICUs (1%). Although the nutritional program is widely prescribed based on the patients' general evaluation, 52 ICUs (52%) do not perform nutritional risk evaluation at admission in case of > 24-h stay. Daily caloric intake is mainly based on the 25 kcal/kg equation; otherwise, the Harris-Benedict formula is mostly used, whereas indirect calorimetry is less used. Most clinicians apply a personalized nutritional approach to organ failure. Most ICUs have a nutritional management protocol, and enteral nutrition (EN) is frequently started within 2 days from admission, while supplemental parenteral nutrition is used when EN is insufficient by most clinicians. The EN administered seems to correspond to that prescribed, but it is stopped if the gastric residual gastric is > 300-500 ml in most ICUs.</p><p><strong>Conclusion: </strong>Prescription, route, and mode of administration of nutritional support seem to be in line with international recommendations, while suggestions on the tools for assessing the nutritional risk and monitoring efficacy and complications seem far less followed. Future national clinical studies are necessary to investigate the optimal nutritional and metabolic management of critically ill patients and the correspondence with the results of this survey on actual practices.</p>","PeriodicalId":73597,"journal":{"name":"Journal of Anesthesia, Analgesia and Critical Care (Online)","volume":"3 1","pages":"45"},"PeriodicalIF":3.1000,"publicationDate":"2023-11-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10631207/pdf/","citationCount":"0","resultStr":"{\"title\":\"Nutritional support and prevention of post-intensive care syndrome: the Italian SIAARTI survey.\",\"authors\":\"Antonella Cotoia, Michele Umbrello, Fiorenza Ferrari, Vincenzo Pota, Francesco Alessandri, Andrea Cortegiani, Silvia De Rosa\",\"doi\":\"10.1186/s44158-023-00132-4\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Malnutrition and muscle wasting are common in ICU patients and predict adverse patient-centered outcomes. The Italian Society of Anesthesia Analgesia Resuscitation and Intensive Care (SIAARTI) conducted a nationwide survey to identify the nutritional practices in the Italian ICUs and to plan future, training interventions to improve the national clinical practice.</p><p><strong>Methods: </strong>Nationwide online survey, involving Italian ICUs, developed by experts affiliated with SIAARTI. Invitations to participate were distributed through emails and social networks. Data were collected over a period of three months (October 1 to December 31, 2022) during 2022.</p><p><strong>Results: </strong>One hundred full responses from participating ICUs were collected. The number of beds is < 10 in most ICUs and > 20 in 11 ICUs. Most ICUs (87%) are mixed, cardiac (5%), neurosurgical (4%), or pediatric ICUs (1%). Although the nutritional program is widely prescribed based on the patients' general evaluation, 52 ICUs (52%) do not perform nutritional risk evaluation at admission in case of > 24-h stay. Daily caloric intake is mainly based on the 25 kcal/kg equation; otherwise, the Harris-Benedict formula is mostly used, whereas indirect calorimetry is less used. Most clinicians apply a personalized nutritional approach to organ failure. Most ICUs have a nutritional management protocol, and enteral nutrition (EN) is frequently started within 2 days from admission, while supplemental parenteral nutrition is used when EN is insufficient by most clinicians. The EN administered seems to correspond to that prescribed, but it is stopped if the gastric residual gastric is > 300-500 ml in most ICUs.</p><p><strong>Conclusion: </strong>Prescription, route, and mode of administration of nutritional support seem to be in line with international recommendations, while suggestions on the tools for assessing the nutritional risk and monitoring efficacy and complications seem far less followed. Future national clinical studies are necessary to investigate the optimal nutritional and metabolic management of critically ill patients and the correspondence with the results of this survey on actual practices.</p>\",\"PeriodicalId\":73597,\"journal\":{\"name\":\"Journal of Anesthesia, Analgesia and Critical Care (Online)\",\"volume\":\"3 1\",\"pages\":\"45\"},\"PeriodicalIF\":3.1000,\"publicationDate\":\"2023-11-07\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10631207/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Anesthesia, Analgesia and Critical Care (Online)\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s44158-023-00132-4\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Anesthesia, Analgesia and Critical Care (Online)","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s44158-023-00132-4","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Nutritional support and prevention of post-intensive care syndrome: the Italian SIAARTI survey.
Background: Malnutrition and muscle wasting are common in ICU patients and predict adverse patient-centered outcomes. The Italian Society of Anesthesia Analgesia Resuscitation and Intensive Care (SIAARTI) conducted a nationwide survey to identify the nutritional practices in the Italian ICUs and to plan future, training interventions to improve the national clinical practice.
Methods: Nationwide online survey, involving Italian ICUs, developed by experts affiliated with SIAARTI. Invitations to participate were distributed through emails and social networks. Data were collected over a period of three months (October 1 to December 31, 2022) during 2022.
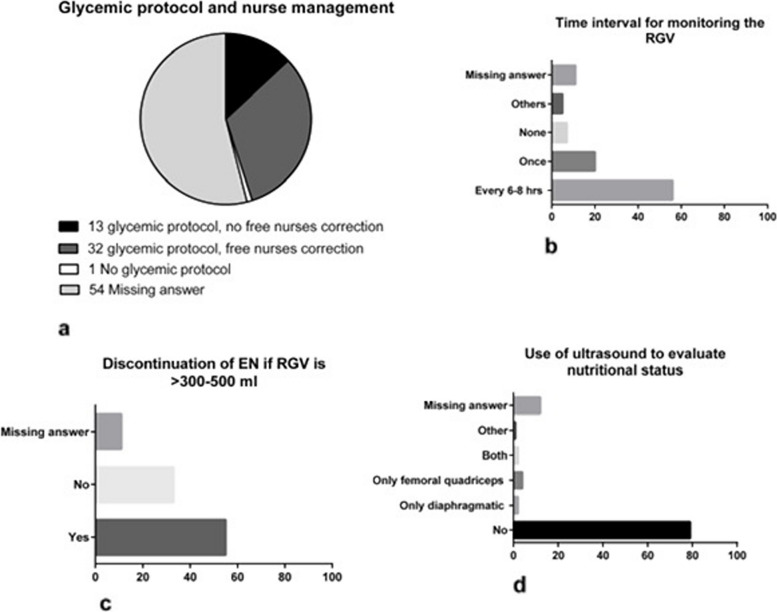
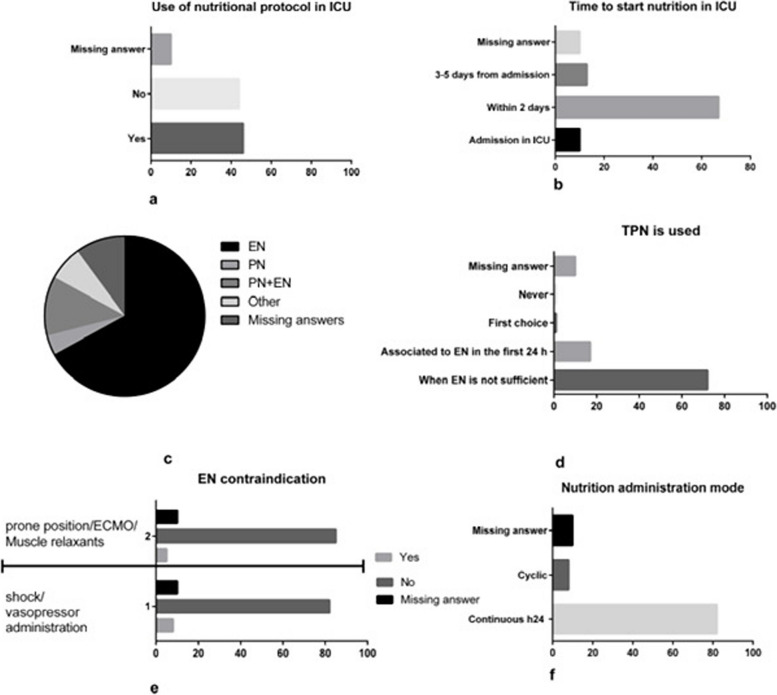
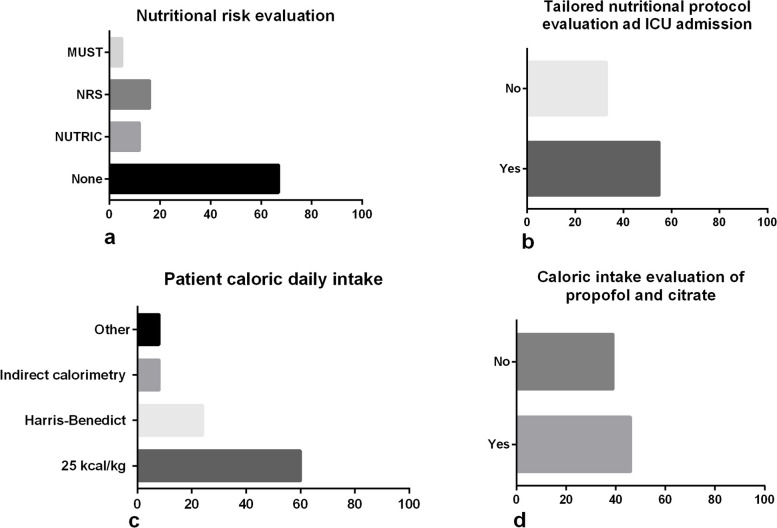
Results: One hundred full responses from participating ICUs were collected. The number of beds is < 10 in most ICUs and > 20 in 11 ICUs. Most ICUs (87%) are mixed, cardiac (5%), neurosurgical (4%), or pediatric ICUs (1%). Although the nutritional program is widely prescribed based on the patients' general evaluation, 52 ICUs (52%) do not perform nutritional risk evaluation at admission in case of > 24-h stay. Daily caloric intake is mainly based on the 25 kcal/kg equation; otherwise, the Harris-Benedict formula is mostly used, whereas indirect calorimetry is less used. Most clinicians apply a personalized nutritional approach to organ failure. Most ICUs have a nutritional management protocol, and enteral nutrition (EN) is frequently started within 2 days from admission, while supplemental parenteral nutrition is used when EN is insufficient by most clinicians. The EN administered seems to correspond to that prescribed, but it is stopped if the gastric residual gastric is > 300-500 ml in most ICUs.
Conclusion: Prescription, route, and mode of administration of nutritional support seem to be in line with international recommendations, while suggestions on the tools for assessing the nutritional risk and monitoring efficacy and complications seem far less followed. Future national clinical studies are necessary to investigate the optimal nutritional and metabolic management of critically ill patients and the correspondence with the results of this survey on actual practices.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
