Paul T R Thiruchelvam, Daniel R Leff, Amy R Godden, Susan Cleator, Simon H Wood, Anna M Kirby, Navid Jallali, Navita Somaiah, Judith E Hunter, Francis P Henry, Aikaterini Micha, Rachel L O'Connell, Kabir Mohammed, Neill Patani, Melissa L H Tan, Dorothy Gujral, Gillian Ross, Stuart E James, Aadil A Khan, Jennifer E Rusby, Dimitri J Hadjiminas, Fiona A MacNeill
{"title":"乳腺癌患者的原位放疗和下腹穿孔带皮瓣重建(PRADA):一项多中心、前瞻性、非随机的可行性研究。","authors":"Paul T R Thiruchelvam, Daniel R Leff, Amy R Godden, Susan Cleator, Simon H Wood, Anna M Kirby, Navid Jallali, Navita Somaiah, Judith E Hunter, Francis P Henry, Aikaterini Micha, Rachel L O'Connell, Kabir Mohammed, Neill Patani, Melissa L H Tan, Dorothy Gujral, Gillian Ross, Stuart E James, Aadil A Khan, Jennifer E Rusby, Dimitri J Hadjiminas, Fiona A MacNeill","doi":"10.1016/S1470-2045(22)00145-0","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Radiotherapy before mastectomy and autologous free-flap breast reconstruction can avoid adverse radiation effects on healthy donor tissues and delays to adjuvant radiotherapy. However, evidence for this treatment sequence is sparse. We aimed to explore the feasibility of preoperative radiotherapy followed by skin-sparing mastectomy and deep inferior epigastric perforator (DIEP) flap reconstruction in patients with breast cancer requiring mastectomy.</p><p><strong>Methods: </strong>We conducted a prospective, non-randomised, feasibility study at two National Health Service trusts in the UK. Eligible patients were women aged older than 18 years with a laboratory diagnosis of primary breast cancer requiring mastectomy and post-mastectomy radiotherapy, who were suitable for DIEP flap reconstruction. Preoperative radiotherapy started 3-4 weeks after neoadjuvant chemotherapy and was delivered to the breast, plus regional nodes as required, at 40 Gy in 15 fractions (over 3 weeks) or 42·72 Gy in 16 fractions (over 3·2 weeks). Adverse skin radiation toxicity was assessed preoperatively using the Radiation Therapy Oncology Group toxicity grading system. Skin-sparing mastectomy and DIEP flap reconstruction were planned for 2-6 weeks after completion of preoperative radiotherapy. The primary endpoint was the proportion of open breast wounds greater than 1 cm width requiring a dressing at 4 weeks after surgery, assessed in all participants. This study is registered with ClinicalTrials.gov, NCT02771938, and is closed to recruitment.</p><p><strong>Findings: </strong>Between Jan 25, 2016, and Dec 11, 2017, 33 patients were enrolled. At 4 weeks after surgery, four (12·1%, 95% CI 3·4-28·2) of 33 patients had an open breast wound greater than 1 cm. One (3%) patient had confluent moist desquamation (grade 3). There were no serious treatment-related adverse events and no treatment-related deaths.</p><p><strong>Interpretation: </strong>Preoperative radiotherapy followed by skin-sparing mastectomy and immediate DIEP flap reconstruction is feasible and technically safe, with rates of breast open wounds similar to those reported with post-mastectomy radiotherapy. A randomised trial comparing preoperative radiotherapy with post-mastectomy radiotherapy is required to precisely determine and compare surgical, oncological, and breast reconstruction outcomes, including quality of life.</p><p><strong>Funding: </strong>Cancer Research UK, National Institute for Health Research.</p>","PeriodicalId":73510,"journal":{"name":"Iranian journal of cancer prevention","volume":"9 1","pages":"682-690"},"PeriodicalIF":0.0000,"publicationDate":"2022-05-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9630150/pdf/","citationCount":"0","resultStr":"{\"title\":\"Primary radiotherapy and deep inferior epigastric perforator flap reconstruction for patients with breast cancer (PRADA): a multicentre, prospective, non-randomised, feasibility study.\",\"authors\":\"Paul T R Thiruchelvam, Daniel R Leff, Amy R Godden, Susan Cleator, Simon H Wood, Anna M Kirby, Navid Jallali, Navita Somaiah, Judith E Hunter, Francis P Henry, Aikaterini Micha, Rachel L O'Connell, Kabir Mohammed, Neill Patani, Melissa L H Tan, Dorothy Gujral, Gillian Ross, Stuart E James, Aadil A Khan, Jennifer E Rusby, Dimitri J Hadjiminas, Fiona A MacNeill\",\"doi\":\"10.1016/S1470-2045(22)00145-0\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Radiotherapy before mastectomy and autologous free-flap breast reconstruction can avoid adverse radiation effects on healthy donor tissues and delays to adjuvant radiotherapy. However, evidence for this treatment sequence is sparse. We aimed to explore the feasibility of preoperative radiotherapy followed by skin-sparing mastectomy and deep inferior epigastric perforator (DIEP) flap reconstruction in patients with breast cancer requiring mastectomy.</p><p><strong>Methods: </strong>We conducted a prospective, non-randomised, feasibility study at two National Health Service trusts in the UK. Eligible patients were women aged older than 18 years with a laboratory diagnosis of primary breast cancer requiring mastectomy and post-mastectomy radiotherapy, who were suitable for DIEP flap reconstruction. Preoperative radiotherapy started 3-4 weeks after neoadjuvant chemotherapy and was delivered to the breast, plus regional nodes as required, at 40 Gy in 15 fractions (over 3 weeks) or 42·72 Gy in 16 fractions (over 3·2 weeks). Adverse skin radiation toxicity was assessed preoperatively using the Radiation Therapy Oncology Group toxicity grading system. Skin-sparing mastectomy and DIEP flap reconstruction were planned for 2-6 weeks after completion of preoperative radiotherapy. The primary endpoint was the proportion of open breast wounds greater than 1 cm width requiring a dressing at 4 weeks after surgery, assessed in all participants. This study is registered with ClinicalTrials.gov, NCT02771938, and is closed to recruitment.</p><p><strong>Findings: </strong>Between Jan 25, 2016, and Dec 11, 2017, 33 patients were enrolled. At 4 weeks after surgery, four (12·1%, 95% CI 3·4-28·2) of 33 patients had an open breast wound greater than 1 cm. One (3%) patient had confluent moist desquamation (grade 3). There were no serious treatment-related adverse events and no treatment-related deaths.</p><p><strong>Interpretation: </strong>Preoperative radiotherapy followed by skin-sparing mastectomy and immediate DIEP flap reconstruction is feasible and technically safe, with rates of breast open wounds similar to those reported with post-mastectomy radiotherapy. A randomised trial comparing preoperative radiotherapy with post-mastectomy radiotherapy is required to precisely determine and compare surgical, oncological, and breast reconstruction outcomes, including quality of life.</p><p><strong>Funding: </strong>Cancer Research UK, National Institute for Health Research.</p>\",\"PeriodicalId\":73510,\"journal\":{\"name\":\"Iranian journal of cancer prevention\",\"volume\":\"9 1\",\"pages\":\"682-690\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2022-05-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9630150/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Iranian journal of cancer prevention\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1016/S1470-2045(22)00145-0\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2022/4/7 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Iranian journal of cancer prevention","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1016/S1470-2045(22)00145-0","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/4/7 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
摘要
背景:在乳房切除术和自体游离瓣乳房重建术前进行放疗,可避免对健康供体组织造成不良辐射影响,也可避免延误辅助放疗。然而,这种治疗顺序的证据并不多。我们的目的是探讨需要进行乳房切除术的乳腺癌患者术前放疗后进行保皮乳房切除术和深下上腹部穿孔器(DIEP)皮瓣重建的可行性:我们在英国两家国民健康服务托管机构开展了一项前瞻性、非随机、可行性研究。符合条件的患者是年龄大于 18 岁、实验室诊断为原发性乳腺癌、需要进行乳房切除术和乳房切除术后放疗、适合进行 DIEP 皮瓣重建术的女性。术前放疗在新辅助化疗后3-4周开始,对乳房及必要的区域结节进行放疗,剂量为40 Gy,15次/分(3周)或42-72 Gy,16次/分(3-2周)。术前采用肿瘤放疗组毒性分级系统对皮肤放射毒性进行评估。计划在术前放疗结束后2-6周进行保皮乳房切除术和DIEP皮瓣重建术。主要终点是所有参与者术后4周时需要敷料的乳房开放性伤口宽度大于1厘米的比例。该研究已在ClinicalTrials.gov注册,编号为NCT02771938,目前已结束招募:2016年1月25日至2017年12月11日期间,33名患者入组。术后4周,33名患者中有4人(12-1%,95% CI 3-4-28-2)的乳房开放性伤口大于1厘米。1名患者(3%)出现汇合性湿性脱屑(3级)。没有发生与治疗相关的严重不良事件,也没有发生与治疗相关的死亡事件:术前放疗后行乳房皮肤保留切除术和即刻DIEP皮瓣重建术是可行的,技术上也是安全的,乳房开放性伤口的发生率与乳房切除术后放疗的发生率相似。需要进行一项随机试验,比较术前放疗和乳房切除术后放疗,以精确确定和比较手术、肿瘤学和乳房重建的结果,包括生活质量:资金来源:英国癌症研究中心、英国国家健康研究所。
Primary radiotherapy and deep inferior epigastric perforator flap reconstruction for patients with breast cancer (PRADA): a multicentre, prospective, non-randomised, feasibility study.
Background: Radiotherapy before mastectomy and autologous free-flap breast reconstruction can avoid adverse radiation effects on healthy donor tissues and delays to adjuvant radiotherapy. However, evidence for this treatment sequence is sparse. We aimed to explore the feasibility of preoperative radiotherapy followed by skin-sparing mastectomy and deep inferior epigastric perforator (DIEP) flap reconstruction in patients with breast cancer requiring mastectomy.
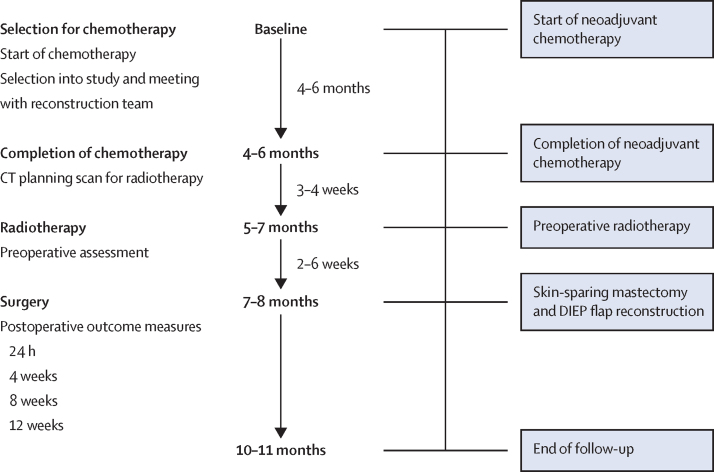
Methods: We conducted a prospective, non-randomised, feasibility study at two National Health Service trusts in the UK. Eligible patients were women aged older than 18 years with a laboratory diagnosis of primary breast cancer requiring mastectomy and post-mastectomy radiotherapy, who were suitable for DIEP flap reconstruction. Preoperative radiotherapy started 3-4 weeks after neoadjuvant chemotherapy and was delivered to the breast, plus regional nodes as required, at 40 Gy in 15 fractions (over 3 weeks) or 42·72 Gy in 16 fractions (over 3·2 weeks). Adverse skin radiation toxicity was assessed preoperatively using the Radiation Therapy Oncology Group toxicity grading system. Skin-sparing mastectomy and DIEP flap reconstruction were planned for 2-6 weeks after completion of preoperative radiotherapy. The primary endpoint was the proportion of open breast wounds greater than 1 cm width requiring a dressing at 4 weeks after surgery, assessed in all participants. This study is registered with ClinicalTrials.gov, NCT02771938, and is closed to recruitment.
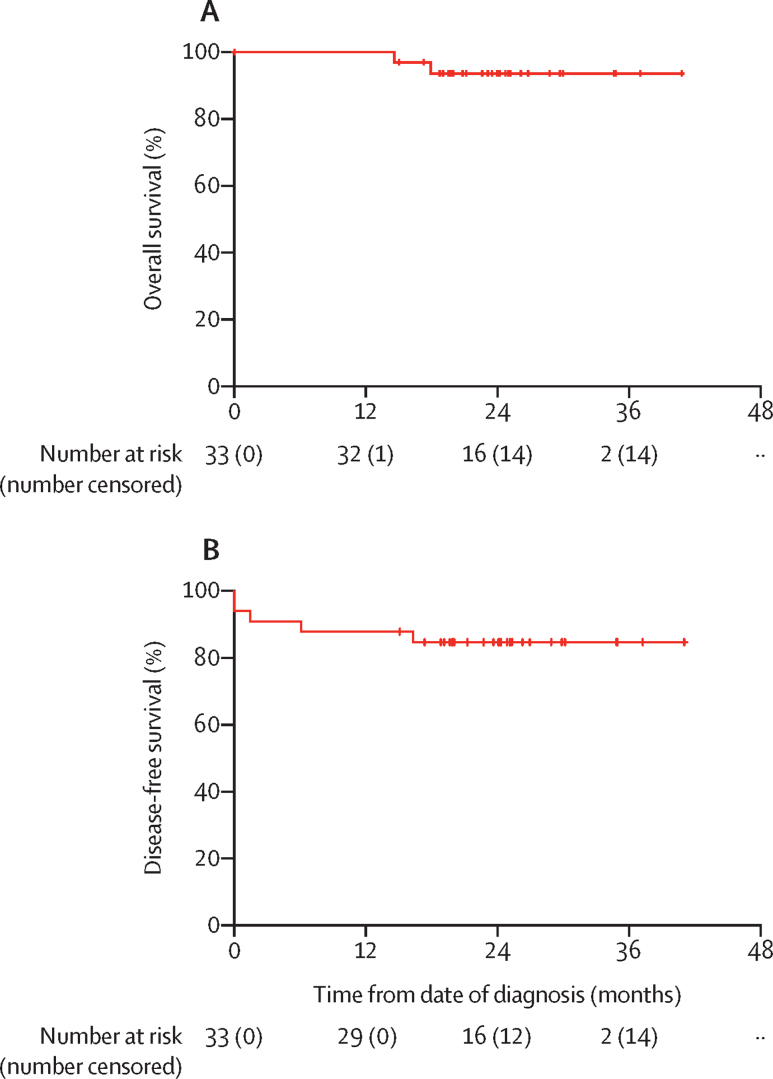
Findings: Between Jan 25, 2016, and Dec 11, 2017, 33 patients were enrolled. At 4 weeks after surgery, four (12·1%, 95% CI 3·4-28·2) of 33 patients had an open breast wound greater than 1 cm. One (3%) patient had confluent moist desquamation (grade 3). There were no serious treatment-related adverse events and no treatment-related deaths.
Interpretation: Preoperative radiotherapy followed by skin-sparing mastectomy and immediate DIEP flap reconstruction is feasible and technically safe, with rates of breast open wounds similar to those reported with post-mastectomy radiotherapy. A randomised trial comparing preoperative radiotherapy with post-mastectomy radiotherapy is required to precisely determine and compare surgical, oncological, and breast reconstruction outcomes, including quality of life.
Funding: Cancer Research UK, National Institute for Health Research.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
