{"title":"即时超声诊断结肠癌。","authors":"Weihao Chen, Readon Teh, Absar Qurishi","doi":"10.24908/pocus.v7i2.15657","DOIUrl":null,"url":null,"abstract":"<p><p>We present a case of a 64-year-old gentleman for whom point of care ultrasound (POCUS) expedited the diagnosis and subsequent early treatment of colon adenocarcinoma. He was referred by his primary provider to our clinic for abdominal bloating. He had no other abdominal symptoms such as abdominal pain, change in bowel habits or rectal bleeding. He had no constitutional symptoms such as weight loss. The patient's abdominal examination was also unremarkable. However, POCUS identified a 6 cm long hypoechoic circumscribed colon wall thickening around the hyperechoic pattern of bowel lumen (Pseudokidney sign)1 in the right upper quadrant, which suggested the presence of an ascending colon carcinoma. In view of this prompt bedside diagnosis, we organised a colonoscopy, staging computerised tomographic scan and colorectal surgery consultation the next day. After the locally advanced colorectal carcinoma was confirmed, the patient had curative surgery within 3 weeks of his presentation to the clinic.</p>","PeriodicalId":74470,"journal":{"name":"POCUS journal","volume":"7 2","pages":"190-192"},"PeriodicalIF":0.0000,"publicationDate":"2022-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9983716/pdf/","citationCount":"0","resultStr":"{\"title\":\"Point-of-Care Ultrasound for the Diagnosis of Colon Cancer.\",\"authors\":\"Weihao Chen, Readon Teh, Absar Qurishi\",\"doi\":\"10.24908/pocus.v7i2.15657\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>We present a case of a 64-year-old gentleman for whom point of care ultrasound (POCUS) expedited the diagnosis and subsequent early treatment of colon adenocarcinoma. He was referred by his primary provider to our clinic for abdominal bloating. He had no other abdominal symptoms such as abdominal pain, change in bowel habits or rectal bleeding. He had no constitutional symptoms such as weight loss. The patient's abdominal examination was also unremarkable. However, POCUS identified a 6 cm long hypoechoic circumscribed colon wall thickening around the hyperechoic pattern of bowel lumen (Pseudokidney sign)1 in the right upper quadrant, which suggested the presence of an ascending colon carcinoma. In view of this prompt bedside diagnosis, we organised a colonoscopy, staging computerised tomographic scan and colorectal surgery consultation the next day. After the locally advanced colorectal carcinoma was confirmed, the patient had curative surgery within 3 weeks of his presentation to the clinic.</p>\",\"PeriodicalId\":74470,\"journal\":{\"name\":\"POCUS journal\",\"volume\":\"7 2\",\"pages\":\"190-192\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2022-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9983716/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"POCUS journal\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.24908/pocus.v7i2.15657\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"POCUS journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.24908/pocus.v7i2.15657","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Point-of-Care Ultrasound for the Diagnosis of Colon Cancer.
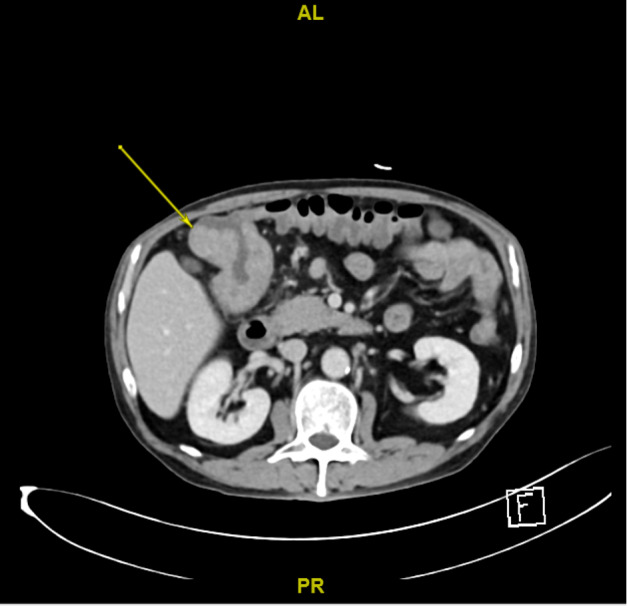
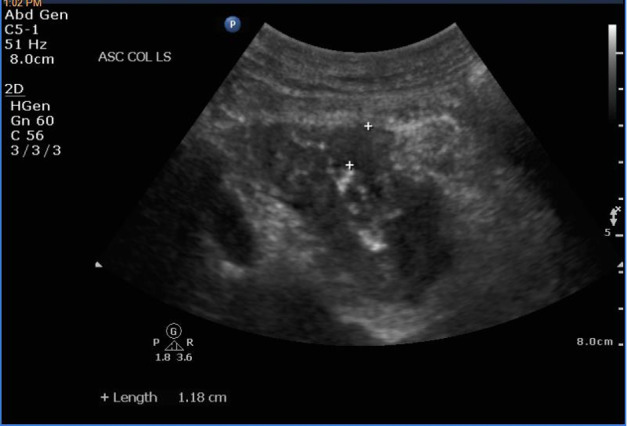
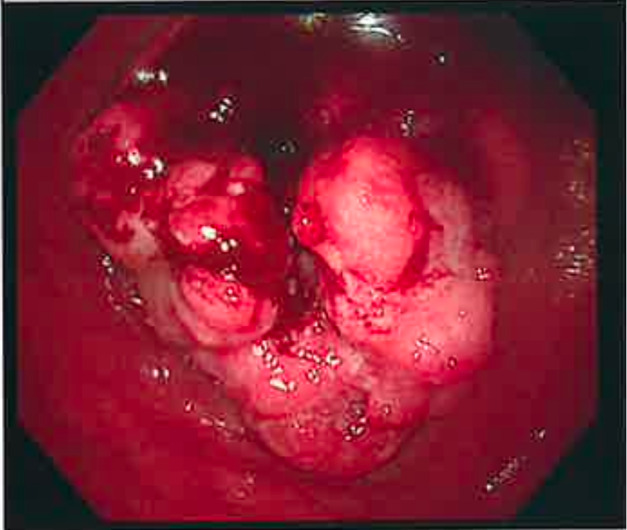
We present a case of a 64-year-old gentleman for whom point of care ultrasound (POCUS) expedited the diagnosis and subsequent early treatment of colon adenocarcinoma. He was referred by his primary provider to our clinic for abdominal bloating. He had no other abdominal symptoms such as abdominal pain, change in bowel habits or rectal bleeding. He had no constitutional symptoms such as weight loss. The patient's abdominal examination was also unremarkable. However, POCUS identified a 6 cm long hypoechoic circumscribed colon wall thickening around the hyperechoic pattern of bowel lumen (Pseudokidney sign)1 in the right upper quadrant, which suggested the presence of an ascending colon carcinoma. In view of this prompt bedside diagnosis, we organised a colonoscopy, staging computerised tomographic scan and colorectal surgery consultation the next day. After the locally advanced colorectal carcinoma was confirmed, the patient had curative surgery within 3 weeks of his presentation to the clinic.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
