{"title":"人工智能辅助软件显著降低了大型辐辏系统中大血管闭塞转运患者的所有工作流程指标。","authors":"Stavros Matsoukas, Laura K Stein, Johanna Fifi","doi":"10.1159/000529077","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Artificial intelligence (AI) software is increasingly applied in stroke diagnostics. Viz LVO (large vessel occlusion) is an AI-based software that is FDA-approved for LVO detection in CT angiography (CTA) scans. We sought to investigate differences in transfer times (from peripheral [spoke] to central [hub] hospitals) for LVO patients between spoke hospitals that utilize Viz LVO and those that do not.</p><p><strong>Methods: </strong>In this retrospective cohort study, we used our institutional database to identify all suspected/confirmed LVO-transferred patients from spokes (peripheral hospitals) within and outside of our healthcare system, from January 2020 to December 2021. The \"Viz-transfers\" group includes all LVO transfers from spokes within our system where Viz LVO is readily available, while the \"Non-Viz-transfers\" group (control group) is comprised of all LVO transfers from spokes outside our system, without Viz LVO. Primary outcome included all available time metrics from peripheral CTA commencement.</p><p><strong>Results: </strong>In total, 78 patients required a transfer. Despite comparable peripheral hospital door to peripheral hospital CTA times (20.5 [24.3] vs. 32 [45] min, p = 0.28) and transfer (spoke to hub) time (23 [18] vs. 26 [13.5], p = 0.763), all workflow metrics were statistically significantly shorter in the Viz-transfers group. Peripheral CTA to interventional neuroradiology team notification was 12 (16.8) versus 58 (59.5), p < 0.001, and peripheral CTA to peripheral departure was 91.5 (37) versus 122.5 (68.5), p < 0.001. Peripheral arrival to peripheral departure was 116.5 (75.5) versus 169 (126.8), p = 0.002, and peripheral arrival to central arrival was 145 (62.5) versus 207 (97.8), p < 0.001. In addition, peripheral CTA to angiosuite arrival was 121 (41) versus 207 (92.5), p < 0.001, peripheral CTA to arterial puncture was 146 (53) versus 234 (99.8), p < 0.001, and peripheral CTA to recanalization was 198 (25) versus 253.5 (86), p < 0.001.</p><p><strong>Conclusion: </strong>Within our spoke and hub system, Viz LVO significantly decreased all workflow metrics for patients who were transferred from spokes with versus without Viz.</p>","PeriodicalId":45709,"journal":{"name":"Cerebrovascular Diseases Extra","volume":" ","pages":"41-46"},"PeriodicalIF":2.1000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/5b/1c/cee-2023-0013-0001-529077.PMC9999083.pdf","citationCount":"0","resultStr":"{\"title\":\"Artificial Intelligence-Assisted Software Significantly Decreases All Workflow Metrics for Large Vessel Occlusion Transfer Patients, within a Large Spoke and Hub System.\",\"authors\":\"Stavros Matsoukas, Laura K Stein, Johanna Fifi\",\"doi\":\"10.1159/000529077\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Artificial intelligence (AI) software is increasingly applied in stroke diagnostics. Viz LVO (large vessel occlusion) is an AI-based software that is FDA-approved for LVO detection in CT angiography (CTA) scans. We sought to investigate differences in transfer times (from peripheral [spoke] to central [hub] hospitals) for LVO patients between spoke hospitals that utilize Viz LVO and those that do not.</p><p><strong>Methods: </strong>In this retrospective cohort study, we used our institutional database to identify all suspected/confirmed LVO-transferred patients from spokes (peripheral hospitals) within and outside of our healthcare system, from January 2020 to December 2021. The \\\"Viz-transfers\\\" group includes all LVO transfers from spokes within our system where Viz LVO is readily available, while the \\\"Non-Viz-transfers\\\" group (control group) is comprised of all LVO transfers from spokes outside our system, without Viz LVO. Primary outcome included all available time metrics from peripheral CTA commencement.</p><p><strong>Results: </strong>In total, 78 patients required a transfer. Despite comparable peripheral hospital door to peripheral hospital CTA times (20.5 [24.3] vs. 32 [45] min, p = 0.28) and transfer (spoke to hub) time (23 [18] vs. 26 [13.5], p = 0.763), all workflow metrics were statistically significantly shorter in the Viz-transfers group. Peripheral CTA to interventional neuroradiology team notification was 12 (16.8) versus 58 (59.5), p < 0.001, and peripheral CTA to peripheral departure was 91.5 (37) versus 122.5 (68.5), p < 0.001. Peripheral arrival to peripheral departure was 116.5 (75.5) versus 169 (126.8), p = 0.002, and peripheral arrival to central arrival was 145 (62.5) versus 207 (97.8), p < 0.001. In addition, peripheral CTA to angiosuite arrival was 121 (41) versus 207 (92.5), p < 0.001, peripheral CTA to arterial puncture was 146 (53) versus 234 (99.8), p < 0.001, and peripheral CTA to recanalization was 198 (25) versus 253.5 (86), p < 0.001.</p><p><strong>Conclusion: </strong>Within our spoke and hub system, Viz LVO significantly decreased all workflow metrics for patients who were transferred from spokes with versus without Viz.</p>\",\"PeriodicalId\":45709,\"journal\":{\"name\":\"Cerebrovascular Diseases Extra\",\"volume\":\" \",\"pages\":\"41-46\"},\"PeriodicalIF\":2.1000,\"publicationDate\":\"2023-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/5b/1c/cee-2023-0013-0001-529077.PMC9999083.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Cerebrovascular Diseases Extra\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1159/000529077\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/2/14 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"PERIPHERAL VASCULAR DISEASE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cerebrovascular Diseases Extra","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1159/000529077","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/2/14 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"PERIPHERAL VASCULAR DISEASE","Score":null,"Total":0}
Artificial Intelligence-Assisted Software Significantly Decreases All Workflow Metrics for Large Vessel Occlusion Transfer Patients, within a Large Spoke and Hub System.
Introduction: Artificial intelligence (AI) software is increasingly applied in stroke diagnostics. Viz LVO (large vessel occlusion) is an AI-based software that is FDA-approved for LVO detection in CT angiography (CTA) scans. We sought to investigate differences in transfer times (from peripheral [spoke] to central [hub] hospitals) for LVO patients between spoke hospitals that utilize Viz LVO and those that do not.
Methods: In this retrospective cohort study, we used our institutional database to identify all suspected/confirmed LVO-transferred patients from spokes (peripheral hospitals) within and outside of our healthcare system, from January 2020 to December 2021. The "Viz-transfers" group includes all LVO transfers from spokes within our system where Viz LVO is readily available, while the "Non-Viz-transfers" group (control group) is comprised of all LVO transfers from spokes outside our system, without Viz LVO. Primary outcome included all available time metrics from peripheral CTA commencement.
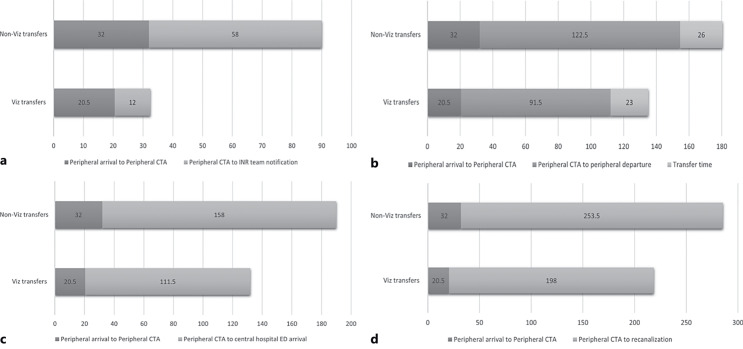
Results: In total, 78 patients required a transfer. Despite comparable peripheral hospital door to peripheral hospital CTA times (20.5 [24.3] vs. 32 [45] min, p = 0.28) and transfer (spoke to hub) time (23 [18] vs. 26 [13.5], p = 0.763), all workflow metrics were statistically significantly shorter in the Viz-transfers group. Peripheral CTA to interventional neuroradiology team notification was 12 (16.8) versus 58 (59.5), p < 0.001, and peripheral CTA to peripheral departure was 91.5 (37) versus 122.5 (68.5), p < 0.001. Peripheral arrival to peripheral departure was 116.5 (75.5) versus 169 (126.8), p = 0.002, and peripheral arrival to central arrival was 145 (62.5) versus 207 (97.8), p < 0.001. In addition, peripheral CTA to angiosuite arrival was 121 (41) versus 207 (92.5), p < 0.001, peripheral CTA to arterial puncture was 146 (53) versus 234 (99.8), p < 0.001, and peripheral CTA to recanalization was 198 (25) versus 253.5 (86), p < 0.001.
Conclusion: Within our spoke and hub system, Viz LVO significantly decreased all workflow metrics for patients who were transferred from spokes with versus without Viz.
期刊介绍:
This open access and online-only journal publishes original articles covering the entire spectrum of stroke and cerebrovascular research, drawing from a variety of specialties such as neurology, internal medicine, surgery, radiology, epidemiology, cardiology, hematology, psychology and rehabilitation. Offering an international forum, it meets the growing need for sophisticated, up-to-date scientific information on clinical data, diagnostic testing, and therapeutic issues. The journal publishes original contributions, reviews of selected topics as well as clinical investigative studies. All aspects related to clinical advances are considered, while purely experimental work appears only if directly relevant to clinical issues. Cerebrovascular Diseases Extra provides additional contents based on reviewed and accepted submissions to the main journal Cerebrovascular Diseases.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
