{"title":"在混合手术室进行有和无灌注不良的 A 型主动脉夹层修复术的中期效果。","authors":"","doi":"10.1053/j.semtcvs.2022.12.003","DOIUrl":null,"url":null,"abstract":"<div><p><span><span>Treatment approach to type A aortic dissection<span> with malperfusion, immediate open aortic repair vs upfront endovascular treatment, remains controversial. From January 2017 to July 2021, 301 consecutive type A repairs were evaluated at our institution. Starting in 2019, all type A aortic dissections were performed in a fixed-fluoroscopy, </span></span>hybrid operating room<span>. Propensity score matching<span> was used to control baseline patient characteristics between traditional and hybrid operating room approaches. There were 144 patients in the traditional group and 157 in the hybrid group. In the hybrid group, 41% (64/157) underwent intraoperative angiograms, and of those, 58% (37/64) received at least 1 endovascular intervention. Following propensity matching, 125 patients remained in each the traditional and hybrid groups. Thirty-day survival was significantly improved in the hybrid cohort at 96.7% (122/125) as compared to the traditional cohort at 87.2% (109/125) (</span></span></span><em>P = 0.</em>002). There were no significant differences in perioperative paralysis (1.6% vs 1.6%, <em>P > 0.</em><span>9), new hemodialysis (12% vs 9.6%, </span><em>P = 0.</em><span>5), fasciotomy (2.4% vs 5.6%, </span><em>P = 0.</em><span>20, and exploratory laparotomy (1.6% vs 4.8%, </span><em>P = 0.</em>3). The hybrid operating room approach to type A aortic dissection, provides the ability to immediately assess distal malperfusion and perform endovascular interventions at the time of open aortic repair, and is associated with significantly higher 30-day and 2-year survival when compared to a stepwise repair approach in a traditional operating room.</p></div>","PeriodicalId":48592,"journal":{"name":"Seminars in Thoracic and Cardiovascular Surgery","volume":"36 3","pages":"Pages 283-291"},"PeriodicalIF":2.5000,"publicationDate":"2024-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":"{\"title\":\"Midterm Outcomes in Type A Aortic Dissection Repair With and Without Malperfusion in a Hybrid Operating Room\",\"authors\":\"\",\"doi\":\"10.1053/j.semtcvs.2022.12.003\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div><p><span><span>Treatment approach to type A aortic dissection<span> with malperfusion, immediate open aortic repair vs upfront endovascular treatment, remains controversial. From January 2017 to July 2021, 301 consecutive type A repairs were evaluated at our institution. Starting in 2019, all type A aortic dissections were performed in a fixed-fluoroscopy, </span></span>hybrid operating room<span>. Propensity score matching<span> was used to control baseline patient characteristics between traditional and hybrid operating room approaches. There were 144 patients in the traditional group and 157 in the hybrid group. In the hybrid group, 41% (64/157) underwent intraoperative angiograms, and of those, 58% (37/64) received at least 1 endovascular intervention. Following propensity matching, 125 patients remained in each the traditional and hybrid groups. Thirty-day survival was significantly improved in the hybrid cohort at 96.7% (122/125) as compared to the traditional cohort at 87.2% (109/125) (</span></span></span><em>P = 0.</em>002). There were no significant differences in perioperative paralysis (1.6% vs 1.6%, <em>P > 0.</em><span>9), new hemodialysis (12% vs 9.6%, </span><em>P = 0.</em><span>5), fasciotomy (2.4% vs 5.6%, </span><em>P = 0.</em><span>20, and exploratory laparotomy (1.6% vs 4.8%, </span><em>P = 0.</em>3). The hybrid operating room approach to type A aortic dissection, provides the ability to immediately assess distal malperfusion and perform endovascular interventions at the time of open aortic repair, and is associated with significantly higher 30-day and 2-year survival when compared to a stepwise repair approach in a traditional operating room.</p></div>\",\"PeriodicalId\":48592,\"journal\":{\"name\":\"Seminars in Thoracic and Cardiovascular Surgery\",\"volume\":\"36 3\",\"pages\":\"Pages 283-291\"},\"PeriodicalIF\":2.5000,\"publicationDate\":\"2024-09-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Seminars in Thoracic and Cardiovascular Surgery\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://www.sciencedirect.com/science/article/pii/S1043067922002805\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2022/12/23 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Seminars in Thoracic and Cardiovascular Surgery","FirstCategoryId":"3","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S1043067922002805","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/12/23 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
摘要
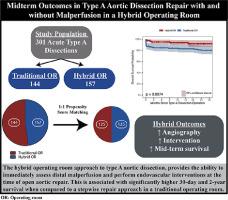
A型主动脉夹层伴灌注不良的治疗方法,即刻开放主动脉修补术与前期血管内治疗,仍存在争议。从 2017 年 1 月到 2021 年 7 月,我院对 301 例连续的 A 型修复术进行了评估。自2019年起,所有A型主动脉夹层均在固定式荧光透视混合手术室进行。采用倾向评分匹配法来控制传统手术室和混合手术室两种方法的患者基线特征。传统组有144名患者,混合组有157名患者。在混合组中,41%(64/157)的患者接受了术中血管造影,其中 58%(37/64)的患者接受了至少一次血管内介入治疗。经过倾向匹配后,传统组和混合组各保留了125名患者。与传统组的87.2%(109/125)相比,混合组的30天存活率明显提高,达到96.7%(122/125)(P = 0.002)。在围手术期瘫痪(1.6% vs 1.6%,P > 0.9)、新的血液透析(12% vs 9.6%,P = 0.5)、筋膜切开术(2.4% vs 5.6%,P = 0.20)和探腹手术(1.6% vs 4.8%,P = 0.3)方面没有明显差异。采用混合手术室方法治疗A型主动脉夹层,能在开腹主动脉修复时立即评估远端灌注不良情况并进行血管内介入治疗,与传统手术室的分步修复方法相比,30天和2年生存率显著提高。
Midterm Outcomes in Type A Aortic Dissection Repair With and Without Malperfusion in a Hybrid Operating Room
Treatment approach to type A aortic dissection with malperfusion, immediate open aortic repair vs upfront endovascular treatment, remains controversial. From January 2017 to July 2021, 301 consecutive type A repairs were evaluated at our institution. Starting in 2019, all type A aortic dissections were performed in a fixed-fluoroscopy, hybrid operating room. Propensity score matching was used to control baseline patient characteristics between traditional and hybrid operating room approaches. There were 144 patients in the traditional group and 157 in the hybrid group. In the hybrid group, 41% (64/157) underwent intraoperative angiograms, and of those, 58% (37/64) received at least 1 endovascular intervention. Following propensity matching, 125 patients remained in each the traditional and hybrid groups. Thirty-day survival was significantly improved in the hybrid cohort at 96.7% (122/125) as compared to the traditional cohort at 87.2% (109/125) (P = 0.002). There were no significant differences in perioperative paralysis (1.6% vs 1.6%, P > 0.9), new hemodialysis (12% vs 9.6%, P = 0.5), fasciotomy (2.4% vs 5.6%, P = 0.20, and exploratory laparotomy (1.6% vs 4.8%, P = 0.3). The hybrid operating room approach to type A aortic dissection, provides the ability to immediately assess distal malperfusion and perform endovascular interventions at the time of open aortic repair, and is associated with significantly higher 30-day and 2-year survival when compared to a stepwise repair approach in a traditional operating room.
期刊介绍:
Seminars in Thoracic and Cardiovascular Surgery is devoted to providing a forum for cardiothoracic surgeons to disseminate and discuss important new information and to gain insight into unresolved areas of question in the specialty. Each issue presents readers with a selection of original peer-reviewed articles accompanied by editorial commentary from specialists in the field. In addition, readers are offered valuable invited articles: State of Views editorials and Current Readings highlighting the latest contributions on central or controversial issues. Another prized feature is expert roundtable discussions in which experts debate critical questions for cardiothoracic treatment and care. Seminars is an invitation-only publication that receives original submissions transferred ONLY from its sister publication, The Journal of Thoracic and Cardiovascular Surgery. As we continue to expand the reach of the Journal, we will explore the possibility of accepting unsolicited manuscripts in the future.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
