Anjana Rajan, Yushan Pan, Prerna Mahtani, Rachel Niec, Randy Longman, Juliette Gerber, Dana Lukin, Ellen Scherl, Robert Battat
{"title":"混杂因素对克罗恩病症状-内窥镜不一致的影响","authors":"Anjana Rajan, Yushan Pan, Prerna Mahtani, Rachel Niec, Randy Longman, Juliette Gerber, Dana Lukin, Ellen Scherl, Robert Battat","doi":"10.1093/crocol/otad017","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Discordances between clinical and endoscopic Crohn's disease (CD) activity indices negatively impact the utility of clinic visits and efficacy assessments in clinical trials. Bile acid diarrhea (BAD) and small intestinal bacterial overgrowth (SIBO) mimic CD symptoms. This study quantified the impact of BAD and SIBO on the relationship between clinical and endoscopic disease activity indices.</p><p><strong>Methods: </strong>CD patients with 7α-hydroxy-4-cholesten-3-one (7C4) serum measurements and/or SIBO breath tests and matched clinical and endoscopic scores were included. Clinical remission (stool frequency [SF] ≤ 1 and abdominal pain score ≤ 1) rates were compared between those with and without (1) endoscopic remission, (2) BAD (7C4 > 55 ng/mL), and (3) SIBO.</p><p><strong>Results: </strong>Of 295 CD patients, 219 had SIBO testing and 87 had 7C4 testing. Patients with elevated 7C4 had lower proportions with clinical remission (14% vs 40%, <i>P</i> = .007) and SF ≤ 1 (14% vs 42%, <i>P</i> = .004) compared to those with normal 7C4. In patients with normal 7C4, higher rates of clinical remission (65% vs 27%, <i>P</i> = .01) and SF ≤ 1 (71% vs 27%, <i>P</i> = .003) existed in patients with endoscopic remission compared to those without endoscopic remission. Conversely, among the entire 295 patient cohorts, nearly identical clinical remission rates existed between those with and without endoscopic remission (25% vs 24%, <i>P</i> = .8), and the Crohn's Disease Patient-Reported Outcome-2 score was not accurate for predicting endoscopic remission (Area Under the Curve (AUC): 0.48; 95% CI, 0.42-0.55). SIBO status did not impact clinical remission rates (<i>P</i> = 1.0).</p><p><strong>Conclusions: </strong>BAD, but not SIBO, contributed to symptom scores. A relationship between endoscopic inflammation and clinical remission rates only existed in patients without 7C4 elevations.</p>","PeriodicalId":10847,"journal":{"name":"Crohn's & Colitis 360","volume":"5 2","pages":"otad017"},"PeriodicalIF":1.8000,"publicationDate":"2023-03-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10066840/pdf/","citationCount":"0","resultStr":"{\"title\":\"The Impact of Confounders on Symptom-Endoscopic Discordances in Crohn's Disease.\",\"authors\":\"Anjana Rajan, Yushan Pan, Prerna Mahtani, Rachel Niec, Randy Longman, Juliette Gerber, Dana Lukin, Ellen Scherl, Robert Battat\",\"doi\":\"10.1093/crocol/otad017\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Discordances between clinical and endoscopic Crohn's disease (CD) activity indices negatively impact the utility of clinic visits and efficacy assessments in clinical trials. Bile acid diarrhea (BAD) and small intestinal bacterial overgrowth (SIBO) mimic CD symptoms. This study quantified the impact of BAD and SIBO on the relationship between clinical and endoscopic disease activity indices.</p><p><strong>Methods: </strong>CD patients with 7α-hydroxy-4-cholesten-3-one (7C4) serum measurements and/or SIBO breath tests and matched clinical and endoscopic scores were included. Clinical remission (stool frequency [SF] ≤ 1 and abdominal pain score ≤ 1) rates were compared between those with and without (1) endoscopic remission, (2) BAD (7C4 > 55 ng/mL), and (3) SIBO.</p><p><strong>Results: </strong>Of 295 CD patients, 219 had SIBO testing and 87 had 7C4 testing. Patients with elevated 7C4 had lower proportions with clinical remission (14% vs 40%, <i>P</i> = .007) and SF ≤ 1 (14% vs 42%, <i>P</i> = .004) compared to those with normal 7C4. In patients with normal 7C4, higher rates of clinical remission (65% vs 27%, <i>P</i> = .01) and SF ≤ 1 (71% vs 27%, <i>P</i> = .003) existed in patients with endoscopic remission compared to those without endoscopic remission. Conversely, among the entire 295 patient cohorts, nearly identical clinical remission rates existed between those with and without endoscopic remission (25% vs 24%, <i>P</i> = .8), and the Crohn's Disease Patient-Reported Outcome-2 score was not accurate for predicting endoscopic remission (Area Under the Curve (AUC): 0.48; 95% CI, 0.42-0.55). SIBO status did not impact clinical remission rates (<i>P</i> = 1.0).</p><p><strong>Conclusions: </strong>BAD, but not SIBO, contributed to symptom scores. A relationship between endoscopic inflammation and clinical remission rates only existed in patients without 7C4 elevations.</p>\",\"PeriodicalId\":10847,\"journal\":{\"name\":\"Crohn's & Colitis 360\",\"volume\":\"5 2\",\"pages\":\"otad017\"},\"PeriodicalIF\":1.8000,\"publicationDate\":\"2023-03-28\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10066840/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Crohn's & Colitis 360\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1093/crocol/otad017\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/4/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Crohn's & Colitis 360","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/crocol/otad017","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/4/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
背景:临床和内镜下克罗恩病(CD)活动指数之间的不一致对临床试验中门诊就诊和疗效评估的效用产生负面影响。胆汁酸腹泻(BAD)和小肠细菌过度生长(SIBO)模拟CD症状。本研究量化BAD和SIBO对临床和内镜下疾病活动性指标之间关系的影响。方法:纳入7α-羟基-4-胆固醇-3-one (7C4)血清测量和/或SIBO呼气测试以及匹配的临床和内镜评分的CD患者。比较有和没有(1)内镜缓解组的临床缓解率(大便频次[SF]≤1和腹痛评分≤1),(2)BAD (7C4 > 55 ng/mL), (3) SIBO。结果:295例CD患者中,219例进行了SIBO检测,87例进行了7C4检测。与7C4正常的患者相比,7C4升高的患者临床缓解的比例(14%对40%,P = 0.007)和SF≤1的比例(14%对42%,P = 0.004)较低。在7C4正常的患者中,内镜下缓解患者的临床缓解率(65% vs 27%, P = 0.01)和SF≤1 (71% vs 27%, P = 0.003)高于非内镜下缓解患者。相反,在整个295名患者队列中,有和没有内窥镜缓解的患者之间存在几乎相同的临床缓解率(25% vs 24%, P = 0.8),克罗恩病患者报告的预后-2评分在预测内窥镜缓解方面并不准确(曲线下面积(AUC): 0.48;95% ci, 0.42-0.55)。SIBO状态不影响临床缓解率(P = 1.0)。结论:BAD对症状评分有影响,而SIBO对症状评分没有影响。内镜下炎症与临床缓解率之间的关系仅存在于没有7C4升高的患者中。
The Impact of Confounders on Symptom-Endoscopic Discordances in Crohn's Disease.
Background: Discordances between clinical and endoscopic Crohn's disease (CD) activity indices negatively impact the utility of clinic visits and efficacy assessments in clinical trials. Bile acid diarrhea (BAD) and small intestinal bacterial overgrowth (SIBO) mimic CD symptoms. This study quantified the impact of BAD and SIBO on the relationship between clinical and endoscopic disease activity indices.
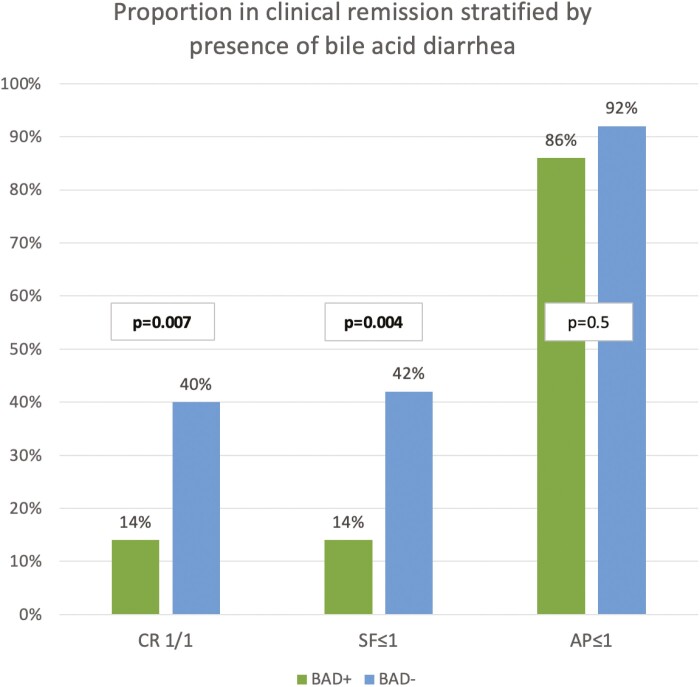
Methods: CD patients with 7α-hydroxy-4-cholesten-3-one (7C4) serum measurements and/or SIBO breath tests and matched clinical and endoscopic scores were included. Clinical remission (stool frequency [SF] ≤ 1 and abdominal pain score ≤ 1) rates were compared between those with and without (1) endoscopic remission, (2) BAD (7C4 > 55 ng/mL), and (3) SIBO.
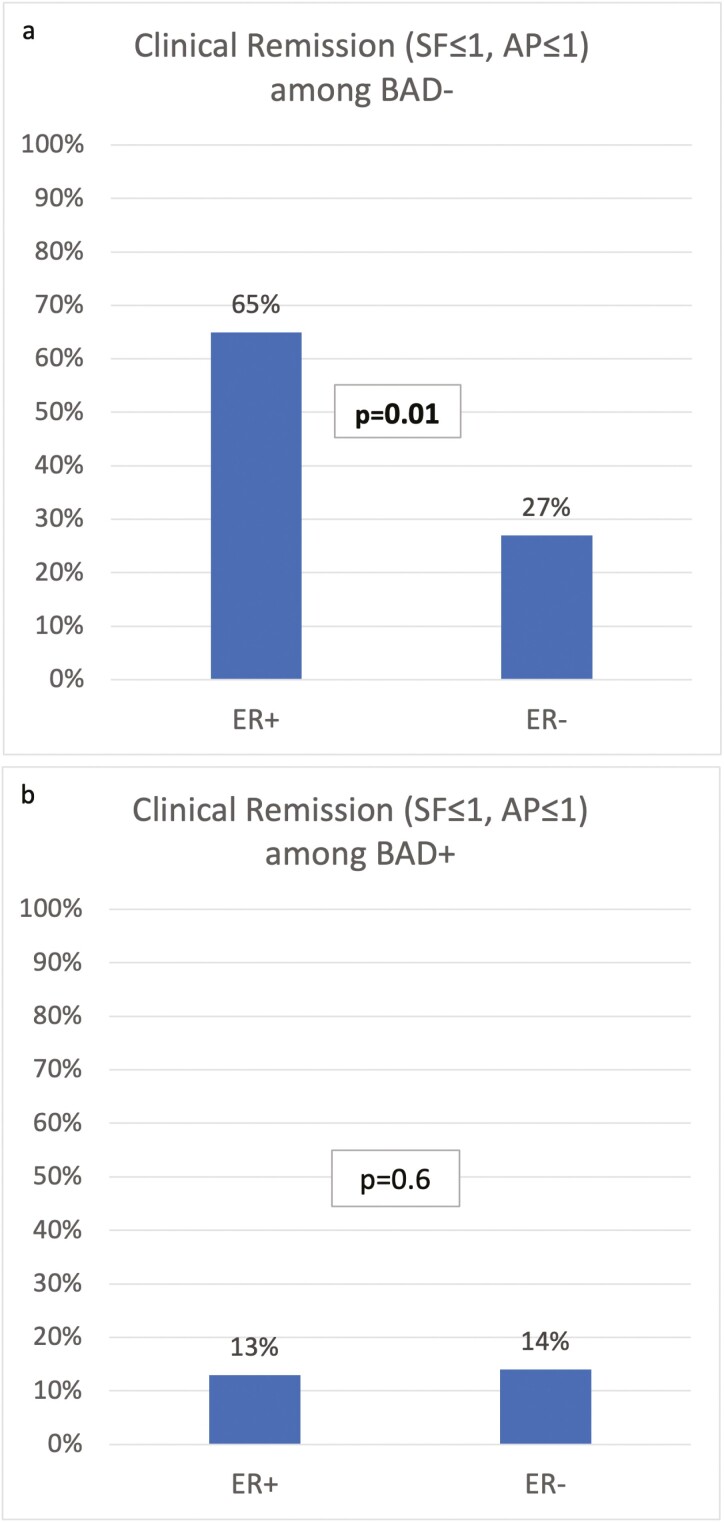
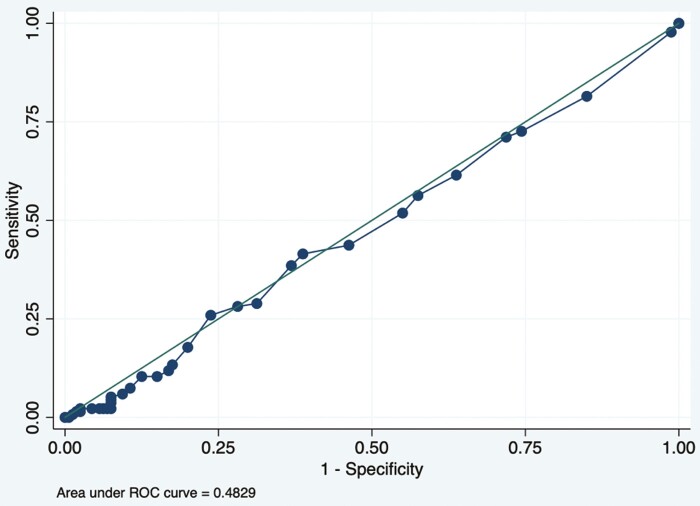
Results: Of 295 CD patients, 219 had SIBO testing and 87 had 7C4 testing. Patients with elevated 7C4 had lower proportions with clinical remission (14% vs 40%, P = .007) and SF ≤ 1 (14% vs 42%, P = .004) compared to those with normal 7C4. In patients with normal 7C4, higher rates of clinical remission (65% vs 27%, P = .01) and SF ≤ 1 (71% vs 27%, P = .003) existed in patients with endoscopic remission compared to those without endoscopic remission. Conversely, among the entire 295 patient cohorts, nearly identical clinical remission rates existed between those with and without endoscopic remission (25% vs 24%, P = .8), and the Crohn's Disease Patient-Reported Outcome-2 score was not accurate for predicting endoscopic remission (Area Under the Curve (AUC): 0.48; 95% CI, 0.42-0.55). SIBO status did not impact clinical remission rates (P = 1.0).
Conclusions: BAD, but not SIBO, contributed to symptom scores. A relationship between endoscopic inflammation and clinical remission rates only existed in patients without 7C4 elevations.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
