Igor Vendramin, Uberto Bortolotti, Aldo D Milano, Ugolino Livi
{"title":"主动脉功能不全手术治疗的曙光。","authors":"Igor Vendramin, Uberto Bortolotti, Aldo D Milano, Ugolino Livi","doi":"10.1111/jocs.16851","DOIUrl":null,"url":null,"abstract":"“Failure is success in progress” ‐ Albert Einstein (1879−1955) Before the development and introduction in the clinical practice of the heart‐lung machine in 1953, to allow intracardiac procedures to be performed under cardiopulmonary bypass (CPB), certain cardiac operations could be accomplished only on a beating heart under mild hypothermia or with the use of cross‐circulation, as utilized by Walton C. Lillehei to successfully repair even complex congenital heart malformations. In 1953, Hufnagel (Figure 1) and Harvey reported the successful implantation of a ball valve prosthesis into the thoracic aorta (Figure 2). This historical operation was performed on September 11, 1952 at Georgetown University Hospital in Washington, DC, in a female patient with severe aortic valve insufficiency. This device, designed to replicate the mechanism of a liquor bottle stopper, produced almost one century ago, consisted in a tubular chamber, with an inlet and an outlet, containing a hollow ball to reduce its gravity; indeed, a pressure of just 5 mmHg was enough to move the poppet in a completely open or closed position. The whole device was molded from a single piece to obtain a smooth surface. Initially, the entire prosthesis was made of methyl methacrylate (Lucite); subsequently the ball was changed with one made by a hollow nylon core covered by silicone rubber to reduce prosthetic noise. As Hufnagel himself stated: “This valve was developed for the treatment of aortic insufficiency and to serve as a prototype to test the possibility that a valvular prosthesis would satisfactorily function within the cardiovascular system.” In those years the CPB machine was still unavailable while replacement of the ascending aorta had not yet been performed. Therefore, Hufnagel was forced to insert this device into the descending aorta and implanting a prosthesis in that location was certainly made possible by the demonstration that the thoracic aorta could be safely temporarily clamped, as occurred during the first landmark operations performed by Robert Gross to close a patent ductus arteriosus or repair an aortic coarctation. The operation to implant the Hufnagel prosthesis was performed through a standard posterolateral thoracotomy incision through the 5th intercostal space with the patient placed in the right lateral decubitus. As described by Hufnagel himself, the prosthesis was implanted in the descending aorta just below the takeoff of the left subclavian artery. Toinsert the prosthesis (Figure 3), following proximal and distal cross‐clamping, a transverse segment of the descending thoracic aorta was excised and the prosthesis inserted into both cut ends of the aorta; the prosthesis was fixed in place using flexible rings at the grooves present on the outer surface at both ends of the valve; occasionally, at the end of the procedure the aorta was wrapped with fabric material. Details of the operation, with some technical modifications, have also been described in the report by Conklin et al. Duration of valve implantation was generally performed in less than 10min since aortic clamping >15min was considered unsafe. Hufnagel reported in 1976 a series of 5 patients operated between 1953 and 1959. Four of these patients underwent subsequently prosthetic aortic valve replacement in the subcoronary position, but the original Hufnagel prosthesis was reported to function well up to 21 years without significant complications related to the original device.","PeriodicalId":15367,"journal":{"name":"Journal of Cardiac Surgery","volume":"37 12","pages":"5676-5678"},"PeriodicalIF":1.3000,"publicationDate":"2022-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10087943/pdf/","citationCount":"2","resultStr":"{\"title\":\"The dawn of surgical treatment of aortic insufficiency.\",\"authors\":\"Igor Vendramin, Uberto Bortolotti, Aldo D Milano, Ugolino Livi\",\"doi\":\"10.1111/jocs.16851\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"“Failure is success in progress” ‐ Albert Einstein (1879−1955) Before the development and introduction in the clinical practice of the heart‐lung machine in 1953, to allow intracardiac procedures to be performed under cardiopulmonary bypass (CPB), certain cardiac operations could be accomplished only on a beating heart under mild hypothermia or with the use of cross‐circulation, as utilized by Walton C. Lillehei to successfully repair even complex congenital heart malformations. In 1953, Hufnagel (Figure 1) and Harvey reported the successful implantation of a ball valve prosthesis into the thoracic aorta (Figure 2). This historical operation was performed on September 11, 1952 at Georgetown University Hospital in Washington, DC, in a female patient with severe aortic valve insufficiency. This device, designed to replicate the mechanism of a liquor bottle stopper, produced almost one century ago, consisted in a tubular chamber, with an inlet and an outlet, containing a hollow ball to reduce its gravity; indeed, a pressure of just 5 mmHg was enough to move the poppet in a completely open or closed position. The whole device was molded from a single piece to obtain a smooth surface. Initially, the entire prosthesis was made of methyl methacrylate (Lucite); subsequently the ball was changed with one made by a hollow nylon core covered by silicone rubber to reduce prosthetic noise. As Hufnagel himself stated: “This valve was developed for the treatment of aortic insufficiency and to serve as a prototype to test the possibility that a valvular prosthesis would satisfactorily function within the cardiovascular system.” In those years the CPB machine was still unavailable while replacement of the ascending aorta had not yet been performed. Therefore, Hufnagel was forced to insert this device into the descending aorta and implanting a prosthesis in that location was certainly made possible by the demonstration that the thoracic aorta could be safely temporarily clamped, as occurred during the first landmark operations performed by Robert Gross to close a patent ductus arteriosus or repair an aortic coarctation. The operation to implant the Hufnagel prosthesis was performed through a standard posterolateral thoracotomy incision through the 5th intercostal space with the patient placed in the right lateral decubitus. As described by Hufnagel himself, the prosthesis was implanted in the descending aorta just below the takeoff of the left subclavian artery. Toinsert the prosthesis (Figure 3), following proximal and distal cross‐clamping, a transverse segment of the descending thoracic aorta was excised and the prosthesis inserted into both cut ends of the aorta; the prosthesis was fixed in place using flexible rings at the grooves present on the outer surface at both ends of the valve; occasionally, at the end of the procedure the aorta was wrapped with fabric material. Details of the operation, with some technical modifications, have also been described in the report by Conklin et al. Duration of valve implantation was generally performed in less than 10min since aortic clamping >15min was considered unsafe. Hufnagel reported in 1976 a series of 5 patients operated between 1953 and 1959. Four of these patients underwent subsequently prosthetic aortic valve replacement in the subcoronary position, but the original Hufnagel prosthesis was reported to function well up to 21 years without significant complications related to the original device.\",\"PeriodicalId\":15367,\"journal\":{\"name\":\"Journal of Cardiac Surgery\",\"volume\":\"37 12\",\"pages\":\"5676-5678\"},\"PeriodicalIF\":1.3000,\"publicationDate\":\"2022-12-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10087943/pdf/\",\"citationCount\":\"2\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Cardiac Surgery\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1111/jocs.16851\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Cardiac Surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1111/jocs.16851","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
The dawn of surgical treatment of aortic insufficiency.
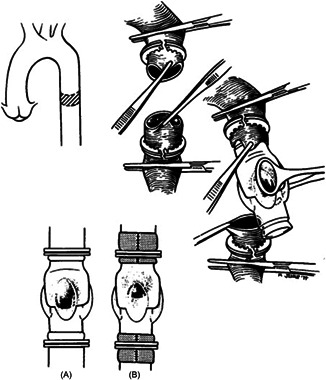
“Failure is success in progress” ‐ Albert Einstein (1879−1955) Before the development and introduction in the clinical practice of the heart‐lung machine in 1953, to allow intracardiac procedures to be performed under cardiopulmonary bypass (CPB), certain cardiac operations could be accomplished only on a beating heart under mild hypothermia or with the use of cross‐circulation, as utilized by Walton C. Lillehei to successfully repair even complex congenital heart malformations. In 1953, Hufnagel (Figure 1) and Harvey reported the successful implantation of a ball valve prosthesis into the thoracic aorta (Figure 2). This historical operation was performed on September 11, 1952 at Georgetown University Hospital in Washington, DC, in a female patient with severe aortic valve insufficiency. This device, designed to replicate the mechanism of a liquor bottle stopper, produced almost one century ago, consisted in a tubular chamber, with an inlet and an outlet, containing a hollow ball to reduce its gravity; indeed, a pressure of just 5 mmHg was enough to move the poppet in a completely open or closed position. The whole device was molded from a single piece to obtain a smooth surface. Initially, the entire prosthesis was made of methyl methacrylate (Lucite); subsequently the ball was changed with one made by a hollow nylon core covered by silicone rubber to reduce prosthetic noise. As Hufnagel himself stated: “This valve was developed for the treatment of aortic insufficiency and to serve as a prototype to test the possibility that a valvular prosthesis would satisfactorily function within the cardiovascular system.” In those years the CPB machine was still unavailable while replacement of the ascending aorta had not yet been performed. Therefore, Hufnagel was forced to insert this device into the descending aorta and implanting a prosthesis in that location was certainly made possible by the demonstration that the thoracic aorta could be safely temporarily clamped, as occurred during the first landmark operations performed by Robert Gross to close a patent ductus arteriosus or repair an aortic coarctation. The operation to implant the Hufnagel prosthesis was performed through a standard posterolateral thoracotomy incision through the 5th intercostal space with the patient placed in the right lateral decubitus. As described by Hufnagel himself, the prosthesis was implanted in the descending aorta just below the takeoff of the left subclavian artery. Toinsert the prosthesis (Figure 3), following proximal and distal cross‐clamping, a transverse segment of the descending thoracic aorta was excised and the prosthesis inserted into both cut ends of the aorta; the prosthesis was fixed in place using flexible rings at the grooves present on the outer surface at both ends of the valve; occasionally, at the end of the procedure the aorta was wrapped with fabric material. Details of the operation, with some technical modifications, have also been described in the report by Conklin et al. Duration of valve implantation was generally performed in less than 10min since aortic clamping >15min was considered unsafe. Hufnagel reported in 1976 a series of 5 patients operated between 1953 and 1959. Four of these patients underwent subsequently prosthetic aortic valve replacement in the subcoronary position, but the original Hufnagel prosthesis was reported to function well up to 21 years without significant complications related to the original device.
期刊介绍:
Journal of Cardiac Surgery (JCS) is a peer-reviewed journal devoted to contemporary surgical treatment of cardiac disease. Renown for its detailed "how to" methods, JCS''s well-illustrated, concise technical articles, critical reviews and commentaries are highly valued by dedicated readers worldwide.
With Editor-in-Chief Harold Lazar, MD and an internationally prominent editorial board, JCS continues its 20-year history as an important professional resource. Editorial coverage includes biologic support, mechanical cardiac assist and/or replacement and surgical techniques, and features current material on topics such as OPCAB surgery, stented and stentless valves, endovascular stent placement, atrial fibrillation, transplantation, percutaneous valve repair/replacement, left ventricular restoration surgery, immunobiology, and bridges to transplant and recovery.
In addition, special sections (Images in Cardiac Surgery, Cardiac Regeneration) and historical reviews stimulate reader interest. The journal also routinely publishes proceedings of important international symposia in a timely manner.





 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
