Amanda Blair Spence, Sameer Desale, Jennifer Lee, Princy Kumar, Xu Huang, Stanley Evan Cooper, Stephen Fernandez, Seble G Kassaye
{"title":"美国艾滋病毒感染者队列中 COVID-19 的结果。","authors":"Amanda Blair Spence, Sameer Desale, Jennifer Lee, Princy Kumar, Xu Huang, Stanley Evan Cooper, Stephen Fernandez, Seble G Kassaye","doi":"10.3390/reports5040041","DOIUrl":null,"url":null,"abstract":"<p><p>Reported coronavirus disease 2019 (COVID-19) outcomes in persons living with HIV (PLWH) vary across cohorts. We examined clinical characteristics and outcomes of PLWH with COVID-19 compared with a matched HIV-seronegative cohort in a mid-Atlantic US healthcare system. Multivariate logistic regression was used to explore factors associated with hospitalization and death/mechanical ventilation among PLWH. Among 281 PLWH with COVID-19, the mean age was 51.5 (SD 12.74) years, 63% were male, 86% were Black, and 87% had a HIV viral load <200 copies/mL. Overall, 47% of PLWH versus 24% (<i>p</i> < 0.001) of matched HIV-seronegative individuals were hospitalized. Rates of COVID-19 associated cardiovascular and thrombotic events, AKI, and infections were similar between PLWH and HIV-seronegative individuals. Overall mortality was 6% (<i>n</i> = 18/281) in PLWH versus 3% (<i>n</i> = 33/1124) HIV-seronegative, <i>p</i> < 0.0001. Among admitted patients, mortality was 14% (<i>n</i> = 18/132) for PLWH and 13% (<i>n</i> = 33/269) for HIV-seronegative, <i>p</i> = 0.75. Among PLWH, hospitalization associated with older age aOR 1.04 (95% CI 1.01, 1.06), Medicaid insurance aOR 2.61 (95% CI 1.39, 4.97) and multimorbidity aOR 2.98 (95% CI 1.72, 5.23). Death/mechanical ventilation associated with older age aOR 1.06 (95% CI 1.01, 1.11), Medicaid insurance aOR 3.6 (95% CI 1.36, 9.74), and multimorbidity aOR 4.4 (95% CI 1.55, 15.9) in adjusted analyses. PLWH were hospitalized more frequently than the HIV-seronegative group and had a higher overall mortality rate, but once hospitalized had similar mortality rates. Older age, multimorbidity and insurance status associated with more severe outcomes among PLWH suggesting the importance of targeted interventions to mitigate the effects of modifiable inequities.</p>","PeriodicalId":74664,"journal":{"name":"Reports (MDPI)","volume":"5 4","pages":""},"PeriodicalIF":0.8000,"publicationDate":"2022-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10104440/pdf/","citationCount":"0","resultStr":"{\"title\":\"COVID-19 Outcomes in a US Cohort of Persons Living with HIV (PLWH).\",\"authors\":\"Amanda Blair Spence, Sameer Desale, Jennifer Lee, Princy Kumar, Xu Huang, Stanley Evan Cooper, Stephen Fernandez, Seble G Kassaye\",\"doi\":\"10.3390/reports5040041\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Reported coronavirus disease 2019 (COVID-19) outcomes in persons living with HIV (PLWH) vary across cohorts. We examined clinical characteristics and outcomes of PLWH with COVID-19 compared with a matched HIV-seronegative cohort in a mid-Atlantic US healthcare system. Multivariate logistic regression was used to explore factors associated with hospitalization and death/mechanical ventilation among PLWH. Among 281 PLWH with COVID-19, the mean age was 51.5 (SD 12.74) years, 63% were male, 86% were Black, and 87% had a HIV viral load <200 copies/mL. Overall, 47% of PLWH versus 24% (<i>p</i> < 0.001) of matched HIV-seronegative individuals were hospitalized. Rates of COVID-19 associated cardiovascular and thrombotic events, AKI, and infections were similar between PLWH and HIV-seronegative individuals. Overall mortality was 6% (<i>n</i> = 18/281) in PLWH versus 3% (<i>n</i> = 33/1124) HIV-seronegative, <i>p</i> < 0.0001. Among admitted patients, mortality was 14% (<i>n</i> = 18/132) for PLWH and 13% (<i>n</i> = 33/269) for HIV-seronegative, <i>p</i> = 0.75. Among PLWH, hospitalization associated with older age aOR 1.04 (95% CI 1.01, 1.06), Medicaid insurance aOR 2.61 (95% CI 1.39, 4.97) and multimorbidity aOR 2.98 (95% CI 1.72, 5.23). Death/mechanical ventilation associated with older age aOR 1.06 (95% CI 1.01, 1.11), Medicaid insurance aOR 3.6 (95% CI 1.36, 9.74), and multimorbidity aOR 4.4 (95% CI 1.55, 15.9) in adjusted analyses. PLWH were hospitalized more frequently than the HIV-seronegative group and had a higher overall mortality rate, but once hospitalized had similar mortality rates. Older age, multimorbidity and insurance status associated with more severe outcomes among PLWH suggesting the importance of targeted interventions to mitigate the effects of modifiable inequities.</p>\",\"PeriodicalId\":74664,\"journal\":{\"name\":\"Reports (MDPI)\",\"volume\":\"5 4\",\"pages\":\"\"},\"PeriodicalIF\":0.8000,\"publicationDate\":\"2022-12-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10104440/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Reports (MDPI)\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.3390/reports5040041\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2022/10/9 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Reports (MDPI)","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3390/reports5040041","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/10/9 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
摘要
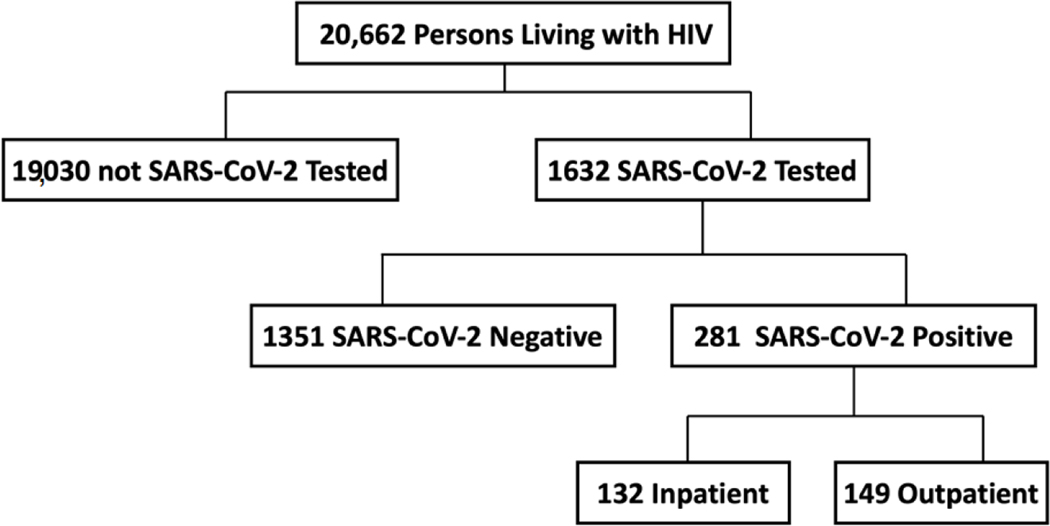
不同队列中报告的艾滋病毒感染者(PLWH)2019 年冠状病毒病(COVID-19)结果各不相同。我们研究了美国大西洋中部医疗系统中感染 COVID-19 的艾滋病病毒感染者与匹配的艾滋病病毒阴性者队列相比的临床特征和结局。我们采用多变量逻辑回归来探讨与感染 COVID-19 的 PLWH 住院和死亡/机械通气相关的因素。在 281 名患有 COVID-19 的 PLWH 中,平均年龄为 51.5(SD 12.74)岁,63% 为男性,86% 为黑人,87% 的匹配 HIV 阴性患者住院治疗。与 COVID-19 相关的心血管和血栓事件、AKI 和感染的发生率在 PLWH 和 HIV 阴性患者之间相似。PLWH 患者的总死亡率为 6%(n = 18/281),而 HIV 阴性患者的总死亡率为 3%(n = 33/1124),P < 0.0001。在住院患者中,PLWH 患者的死亡率为 14%(n = 18/132),HIV 阴性患者的死亡率为 13%(n = 33/269),p = 0.75。在 PLWH 患者中,住院与年龄较大 aOR 1.04 (95% CI 1.01, 1.06)、医疗补助保险 aOR 2.61 (95% CI 1.39, 4.97)和多病相关 aOR 2.98 (95% CI 1.72, 5.23)。在调整分析中,死亡/机械通气与年龄较大 aOR 1.06(95% CI 1.01,1.11)、医疗补助保险 aOR 3.6(95% CI 1.36,9.74)和多病症 aOR 4.4(95% CI 1.55,15.9)相关。与艾滋病毒阴性组相比,艾滋病毒携带者住院的频率更高,总死亡率也更高,但一旦住院,死亡率却相差无几。高龄、多病和保险状况与艾滋病毒感染者更严重的结果有关,这表明采取有针对性的干预措施以减轻可改变的不平等的影响非常重要。
COVID-19 Outcomes in a US Cohort of Persons Living with HIV (PLWH).
Reported coronavirus disease 2019 (COVID-19) outcomes in persons living with HIV (PLWH) vary across cohorts. We examined clinical characteristics and outcomes of PLWH with COVID-19 compared with a matched HIV-seronegative cohort in a mid-Atlantic US healthcare system. Multivariate logistic regression was used to explore factors associated with hospitalization and death/mechanical ventilation among PLWH. Among 281 PLWH with COVID-19, the mean age was 51.5 (SD 12.74) years, 63% were male, 86% were Black, and 87% had a HIV viral load <200 copies/mL. Overall, 47% of PLWH versus 24% (p < 0.001) of matched HIV-seronegative individuals were hospitalized. Rates of COVID-19 associated cardiovascular and thrombotic events, AKI, and infections were similar between PLWH and HIV-seronegative individuals. Overall mortality was 6% (n = 18/281) in PLWH versus 3% (n = 33/1124) HIV-seronegative, p < 0.0001. Among admitted patients, mortality was 14% (n = 18/132) for PLWH and 13% (n = 33/269) for HIV-seronegative, p = 0.75. Among PLWH, hospitalization associated with older age aOR 1.04 (95% CI 1.01, 1.06), Medicaid insurance aOR 2.61 (95% CI 1.39, 4.97) and multimorbidity aOR 2.98 (95% CI 1.72, 5.23). Death/mechanical ventilation associated with older age aOR 1.06 (95% CI 1.01, 1.11), Medicaid insurance aOR 3.6 (95% CI 1.36, 9.74), and multimorbidity aOR 4.4 (95% CI 1.55, 15.9) in adjusted analyses. PLWH were hospitalized more frequently than the HIV-seronegative group and had a higher overall mortality rate, but once hospitalized had similar mortality rates. Older age, multimorbidity and insurance status associated with more severe outcomes among PLWH suggesting the importance of targeted interventions to mitigate the effects of modifiable inequities.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
