{"title":"在2019-2022年SARS-CoV-2大流行之前和期间推出抗生素管理干预措施的单中心经验。","authors":"Zahra Kassamali Escobar, Todd Bouchard, Cameron Buck, Kamaldeep Sandhu, Chloe Bryson-Cahn","doi":"10.7573/dic.2022-7-5","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Antibiotics are prescribed to nearly one-half of patients with viral respiratory tract infections (RTI) in outpatient settings. This use is ineffective and may cause undue harm and excess cost from unnecessary antibiotic exposure. We implemented a multifaceted intervention to address inappropriate antibiotic prescribing for viral RTI. Here, we discuss the impact over 4 years, before and during the SARS-CoV-2 pandemic.</p><p><strong>Methods: </strong>This observational study describes the implementation and initial impact of a multimodal stewardship intervention on inappropriate antibiotic prescribing for viral RTIs in outpatient care settings at a single centre. We tracked the rate of visits for viral RTI as well as antibiotic prescribing for viral RTIs in urgent care, primary care and the emergency department between January 2018 and March 2022. Data were collected 1 year prior to implementation and 3 years after implementation. The primary outcome - the rate of inappropriate antibiotics prescribed for viral RTIs - was described by calendar year (CY) to review changes after the stewardship intervention.</p><p><strong>Results: </strong>In CY2018, the year prior to implementation of targeted RTI antimicrobial stewardship, the rate of inappropriate RTI antibiotics prescribed was 10% in urgent care, 11% in primary care and 18% in the emergency department (ED). During the first CY of the intervention, rates were 8% in urgent care, 10% in primary care and 16% in the ED. In CY2020, the second year of the intervention, inappropriate RTI antibiotics were prescribed in 5% of urgent care and 3% primary care RTI visits and 15% of ED RTI visits. These rates were similar in CY2021 and the first 3 months of CY2022. Over 30,000 visits for RTIs were seen annually in CY2018 and CY2019. Annual RTI visits dropped to 20,222 in CY2020 and 14,172 in CY2021.</p><p><strong>Conclusion: </strong>Although total visits for non-COVID RTIs decreased by approximately 50% during the first 2 years of the SARS-CoV-2 pandemic, an antimicrobial stewardship intervention was associated with decreases in inappropriate antibiotic prescribing for RTIs. This was maintained throughout 2 years of the pandemic.This article is part of the <i>Antibiotic stewardship</i> Special Issue: https://www.drugsincontext.com/special_issues/antimicrobial-stewardship-a-focus-on-the-need-for-moderation.</p>","PeriodicalId":11362,"journal":{"name":"Drugs in Context","volume":"12 ","pages":""},"PeriodicalIF":2.8000,"publicationDate":"2023-02-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/13/48/dic-2022-7-5.PMC9949760.pdf","citationCount":"0","resultStr":"{\"title\":\"A single-centre experience rolling out an antibiotic stewardship intervention prior to and during the SARS-CoV-2 pandemic 2019-2022.\",\"authors\":\"Zahra Kassamali Escobar, Todd Bouchard, Cameron Buck, Kamaldeep Sandhu, Chloe Bryson-Cahn\",\"doi\":\"10.7573/dic.2022-7-5\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Antibiotics are prescribed to nearly one-half of patients with viral respiratory tract infections (RTI) in outpatient settings. This use is ineffective and may cause undue harm and excess cost from unnecessary antibiotic exposure. We implemented a multifaceted intervention to address inappropriate antibiotic prescribing for viral RTI. Here, we discuss the impact over 4 years, before and during the SARS-CoV-2 pandemic.</p><p><strong>Methods: </strong>This observational study describes the implementation and initial impact of a multimodal stewardship intervention on inappropriate antibiotic prescribing for viral RTIs in outpatient care settings at a single centre. We tracked the rate of visits for viral RTI as well as antibiotic prescribing for viral RTIs in urgent care, primary care and the emergency department between January 2018 and March 2022. Data were collected 1 year prior to implementation and 3 years after implementation. The primary outcome - the rate of inappropriate antibiotics prescribed for viral RTIs - was described by calendar year (CY) to review changes after the stewardship intervention.</p><p><strong>Results: </strong>In CY2018, the year prior to implementation of targeted RTI antimicrobial stewardship, the rate of inappropriate RTI antibiotics prescribed was 10% in urgent care, 11% in primary care and 18% in the emergency department (ED). During the first CY of the intervention, rates were 8% in urgent care, 10% in primary care and 16% in the ED. In CY2020, the second year of the intervention, inappropriate RTI antibiotics were prescribed in 5% of urgent care and 3% primary care RTI visits and 15% of ED RTI visits. These rates were similar in CY2021 and the first 3 months of CY2022. Over 30,000 visits for RTIs were seen annually in CY2018 and CY2019. Annual RTI visits dropped to 20,222 in CY2020 and 14,172 in CY2021.</p><p><strong>Conclusion: </strong>Although total visits for non-COVID RTIs decreased by approximately 50% during the first 2 years of the SARS-CoV-2 pandemic, an antimicrobial stewardship intervention was associated with decreases in inappropriate antibiotic prescribing for RTIs. This was maintained throughout 2 years of the pandemic.This article is part of the <i>Antibiotic stewardship</i> Special Issue: https://www.drugsincontext.com/special_issues/antimicrobial-stewardship-a-focus-on-the-need-for-moderation.</p>\",\"PeriodicalId\":11362,\"journal\":{\"name\":\"Drugs in Context\",\"volume\":\"12 \",\"pages\":\"\"},\"PeriodicalIF\":2.8000,\"publicationDate\":\"2023-02-20\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/13/48/dic-2022-7-5.PMC9949760.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Drugs in Context\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.7573/dic.2022-7-5\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"Pharmacology, Toxicology and Pharmaceutics\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Drugs in Context","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.7573/dic.2022-7-5","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"Pharmacology, Toxicology and Pharmaceutics","Score":null,"Total":0}
A single-centre experience rolling out an antibiotic stewardship intervention prior to and during the SARS-CoV-2 pandemic 2019-2022.
Background: Antibiotics are prescribed to nearly one-half of patients with viral respiratory tract infections (RTI) in outpatient settings. This use is ineffective and may cause undue harm and excess cost from unnecessary antibiotic exposure. We implemented a multifaceted intervention to address inappropriate antibiotic prescribing for viral RTI. Here, we discuss the impact over 4 years, before and during the SARS-CoV-2 pandemic.
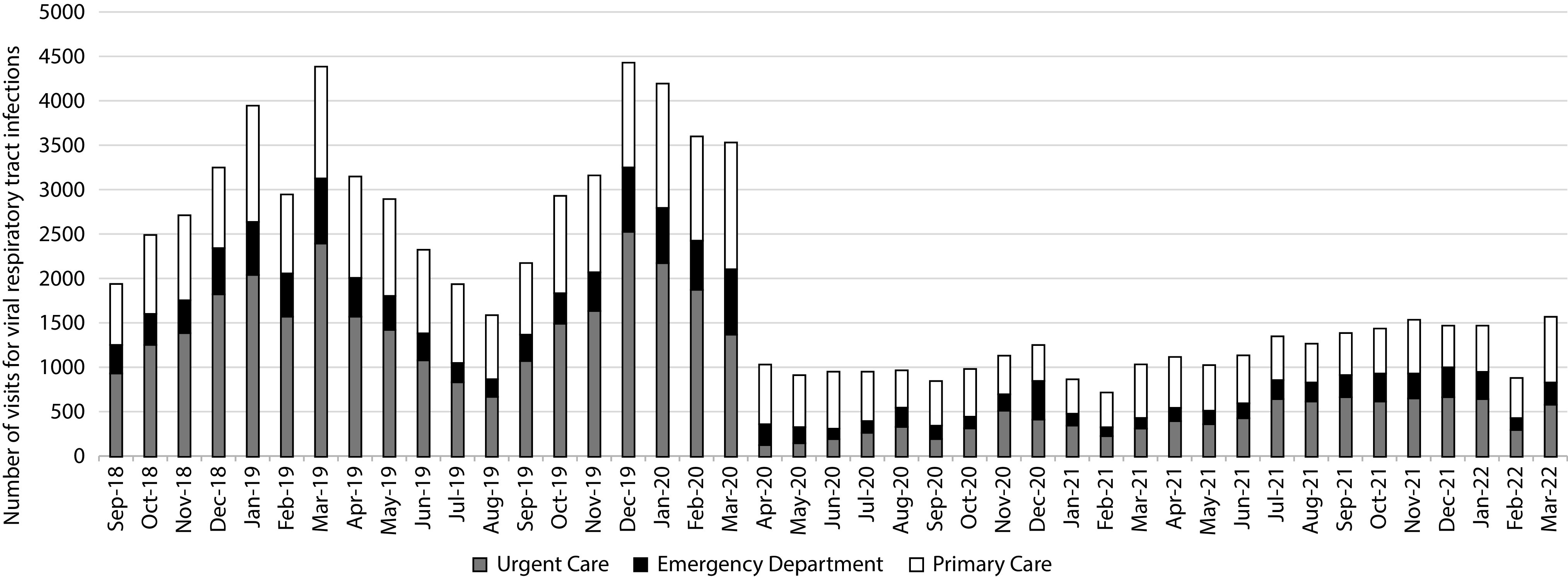
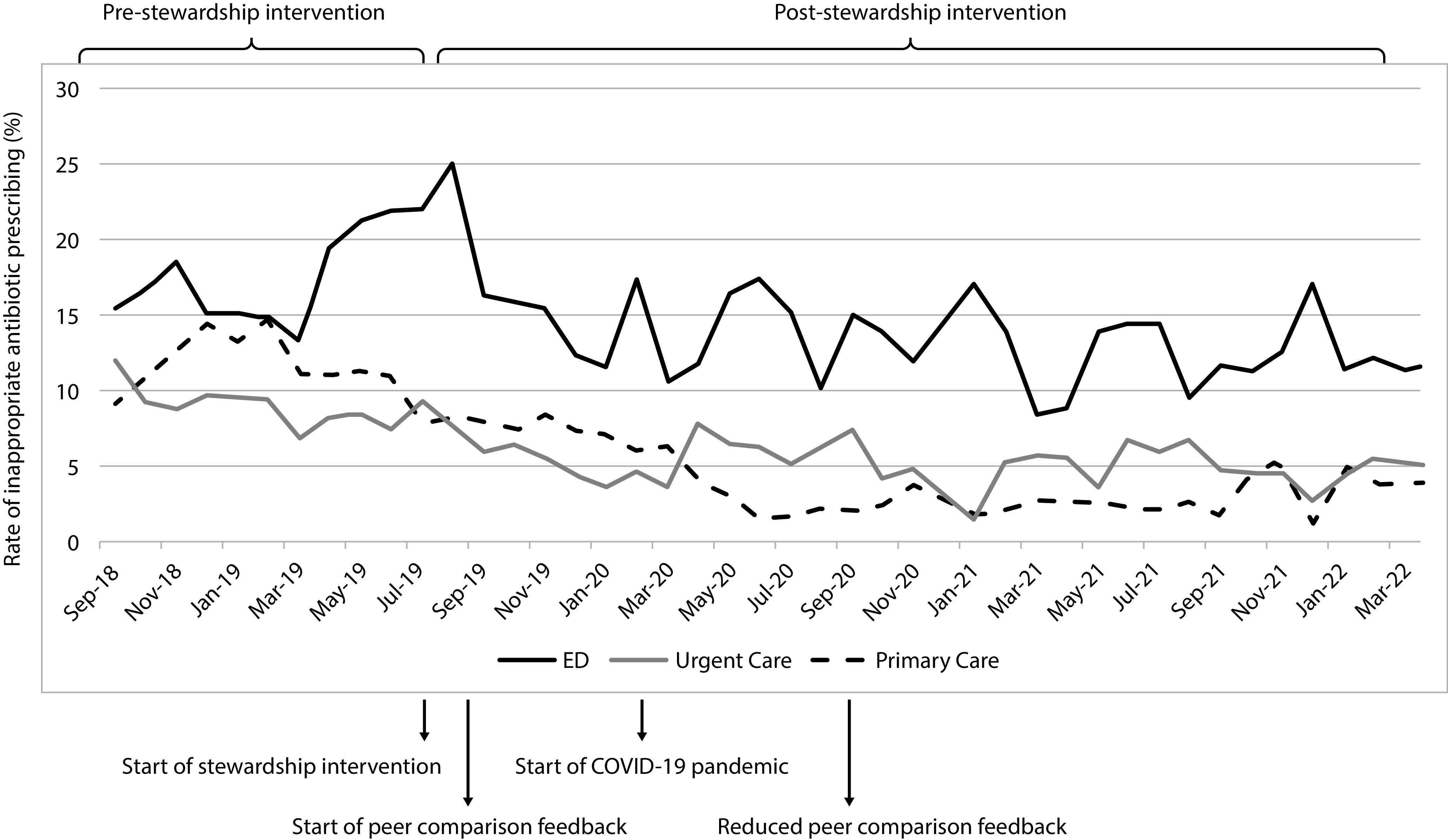
Methods: This observational study describes the implementation and initial impact of a multimodal stewardship intervention on inappropriate antibiotic prescribing for viral RTIs in outpatient care settings at a single centre. We tracked the rate of visits for viral RTI as well as antibiotic prescribing for viral RTIs in urgent care, primary care and the emergency department between January 2018 and March 2022. Data were collected 1 year prior to implementation and 3 years after implementation. The primary outcome - the rate of inappropriate antibiotics prescribed for viral RTIs - was described by calendar year (CY) to review changes after the stewardship intervention.
Results: In CY2018, the year prior to implementation of targeted RTI antimicrobial stewardship, the rate of inappropriate RTI antibiotics prescribed was 10% in urgent care, 11% in primary care and 18% in the emergency department (ED). During the first CY of the intervention, rates were 8% in urgent care, 10% in primary care and 16% in the ED. In CY2020, the second year of the intervention, inappropriate RTI antibiotics were prescribed in 5% of urgent care and 3% primary care RTI visits and 15% of ED RTI visits. These rates were similar in CY2021 and the first 3 months of CY2022. Over 30,000 visits for RTIs were seen annually in CY2018 and CY2019. Annual RTI visits dropped to 20,222 in CY2020 and 14,172 in CY2021.
Conclusion: Although total visits for non-COVID RTIs decreased by approximately 50% during the first 2 years of the SARS-CoV-2 pandemic, an antimicrobial stewardship intervention was associated with decreases in inappropriate antibiotic prescribing for RTIs. This was maintained throughout 2 years of the pandemic.This article is part of the Antibiotic stewardship Special Issue: https://www.drugsincontext.com/special_issues/antimicrobial-stewardship-a-focus-on-the-need-for-moderation.
期刊介绍:
Covers all phases of original research: laboratory, animal and human/clinical studies, health economics and outcomes research, and postmarketing studies. Original research that shows positive or negative results are welcomed. Invited review articles may cover single-drug reviews, drug class reviews, latest advances in drug therapy, therapeutic-area reviews, place-in-therapy reviews, new pathways and classes of drugs. In addition, systematic reviews and meta-analyses are welcomed and may be published as original research if performed per accepted guidelines. Editorials of key topics and issues in drugs and therapeutics are welcomed. The Editor-in-Chief will also consider manuscripts of interest in areas such as technologies that support diagnosis, assessment and treatment. EQUATOR Network reporting guidelines should be followed for each article type. GPP3 Guidelines should be followed for any industry-sponsored manuscripts. Other Editorial sections may include Editorial, Case Report, Conference Report, Letter-to-the-Editor, Educational Section.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
