Dylan Edwards, Sapna Kumar, Lorie Brinkman, Isabel Cardoso Ferreira, Alberto Esquenazi, Tiffany Nguyen, Michael Su, Stephanie Stein, Jaun May, Allison Hendrix, Casey Finley, Emily Howard, Steven C Cramer
{"title":"脑卒中后早期远程康复的可行性研究。","authors":"Dylan Edwards, Sapna Kumar, Lorie Brinkman, Isabel Cardoso Ferreira, Alberto Esquenazi, Tiffany Nguyen, Michael Su, Stephanie Stein, Jaun May, Allison Hendrix, Casey Finley, Emily Howard, Steven C Cramer","doi":"10.1177/15459683231159660","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Enhanced neural plasticity early after stroke suggests the potential to improve outcomes with intensive rehabilitation therapy. Most patients do not get such therapy, however, due to limited access, changing rehabilitation therapy settings, low therapy doses, and poor compliance.</p><p><strong>Objective: </strong>To examine the feasibility, safety, and potential efficacy of an established telerehabilitation (TR) program after stroke initiated during admission to an inpatient rehabilitation facility (IRF) and completed in the patient's home.</p><p><strong>Methods: </strong>Participants with hemiparetic stroke admitted to an IRF received daily TR targeting arm motor function in addition to usual care. Treatment consisted of 36, 70-minute sessions (half supervised by a licensed therapist via videoconference), over a 6-week period, that included functional games, exercise videos, education, and daily assessments.</p><p><strong>Results: </strong>Sixteen participants of 19 allocated completed the intervention (age 61.3 ± 9.4 years; 6 female; baseline Upper Extremity Fugl-Meyer [UEFM] score 35.9 ± 6.4 points, mean ± SD; NIHSS score 4 (3.75, 5.25), median, IQR; intervention commenced 28.3 ± 13.0 days post-stroke). Compliance was 100%, retention 84%, and patient satisfaction 93%; 2 patients developed COVID-19 and continued TR. Post-intervention UEFM improvement was 18.1 ± 10.9 points (<i>P</i> < .0001); Box and Blocks, 22.4 ± 9.8 blocks (<i>P</i> = .0001). Digital motor assessments, acquired daily in the home, were concordant with these gains. The dose of rehabilitation therapy received as usual care during this 6-week interval was 33.9 ± 20.3 hours; adding TR more than doubled this to 73.6 ± 21.8 hours (<i>P</i> < .0001). Patients enrolled in Philadelphia could be treated remotely by therapists in Los Angeles.</p><p><strong>Conclusions: </strong>These results support feasibility, safety, and potential efficacy of providing intense TR therapy early after stroke.</p><p><strong>Clinical trial registration: </strong>clinicaltrials.gov; NCT04657770.</p>","PeriodicalId":56104,"journal":{"name":"Neurorehabilitation and Neural Repair","volume":"37 2-3","pages":"131-141"},"PeriodicalIF":4.0000,"publicationDate":"2023-02-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10080366/pdf/","citationCount":"4","resultStr":"{\"title\":\"Telerehabilitation Initiated Early in Post-Stroke Recovery: A Feasibility Study.\",\"authors\":\"Dylan Edwards, Sapna Kumar, Lorie Brinkman, Isabel Cardoso Ferreira, Alberto Esquenazi, Tiffany Nguyen, Michael Su, Stephanie Stein, Jaun May, Allison Hendrix, Casey Finley, Emily Howard, Steven C Cramer\",\"doi\":\"10.1177/15459683231159660\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Enhanced neural plasticity early after stroke suggests the potential to improve outcomes with intensive rehabilitation therapy. Most patients do not get such therapy, however, due to limited access, changing rehabilitation therapy settings, low therapy doses, and poor compliance.</p><p><strong>Objective: </strong>To examine the feasibility, safety, and potential efficacy of an established telerehabilitation (TR) program after stroke initiated during admission to an inpatient rehabilitation facility (IRF) and completed in the patient's home.</p><p><strong>Methods: </strong>Participants with hemiparetic stroke admitted to an IRF received daily TR targeting arm motor function in addition to usual care. Treatment consisted of 36, 70-minute sessions (half supervised by a licensed therapist via videoconference), over a 6-week period, that included functional games, exercise videos, education, and daily assessments.</p><p><strong>Results: </strong>Sixteen participants of 19 allocated completed the intervention (age 61.3 ± 9.4 years; 6 female; baseline Upper Extremity Fugl-Meyer [UEFM] score 35.9 ± 6.4 points, mean ± SD; NIHSS score 4 (3.75, 5.25), median, IQR; intervention commenced 28.3 ± 13.0 days post-stroke). Compliance was 100%, retention 84%, and patient satisfaction 93%; 2 patients developed COVID-19 and continued TR. Post-intervention UEFM improvement was 18.1 ± 10.9 points (<i>P</i> < .0001); Box and Blocks, 22.4 ± 9.8 blocks (<i>P</i> = .0001). Digital motor assessments, acquired daily in the home, were concordant with these gains. The dose of rehabilitation therapy received as usual care during this 6-week interval was 33.9 ± 20.3 hours; adding TR more than doubled this to 73.6 ± 21.8 hours (<i>P</i> < .0001). Patients enrolled in Philadelphia could be treated remotely by therapists in Los Angeles.</p><p><strong>Conclusions: </strong>These results support feasibility, safety, and potential efficacy of providing intense TR therapy early after stroke.</p><p><strong>Clinical trial registration: </strong>clinicaltrials.gov; NCT04657770.</p>\",\"PeriodicalId\":56104,\"journal\":{\"name\":\"Neurorehabilitation and Neural Repair\",\"volume\":\"37 2-3\",\"pages\":\"131-141\"},\"PeriodicalIF\":4.0000,\"publicationDate\":\"2023-02-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10080366/pdf/\",\"citationCount\":\"4\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Neurorehabilitation and Neural Repair\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1177/15459683231159660\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"CLINICAL NEUROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Neurorehabilitation and Neural Repair","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/15459683231159660","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 4
摘要
背景:脑卒中后早期增强的神经可塑性表明强化康复治疗可能改善预后。然而,由于获取途径有限、不断变化的康复治疗环境、低治疗剂量和较差的依从性,大多数患者没有得到这种治疗。目的:探讨卒中患者在住院康复机构(IRF)住院期间开始远程康复(TR)并在家中完成远程康复(TR)计划的可行性、安全性和潜在疗效。方法:接受IRF治疗的偏瘫性卒中患者除了常规护理外,每天接受针对手臂运动功能的TR。治疗包括36,70分钟的疗程(一半由有执照的治疗师通过视频会议监督),为期6周,包括功能游戏,运动视频,教育和日常评估。结果:19名受试者中有16名完成了干预(年龄61.3±9.4岁;6女;基线上肢Fugl-Meyer评分35.9±6.4分,平均值±SD;NIHSS评分4(3.75,5.25),中位数,IQR;中风后28.3±13.0天开始干预。依从性100%,保留率84%,患者满意度93%;2例患者发生新冠肺炎,并持续TR。干预后UEFM改善18.1±10.9分(P P = 0.0001)。每天在家中获得的数字运动评估与这些成果相一致。在这6周的间隔时间内,接受常规康复治疗的剂量为33.9±20.3小时;结论:这些结果支持卒中后早期提供高强度TR治疗的可行性、安全性和潜在疗效。临床试验注册:clinicaltrials.gov;NCT04657770。
Telerehabilitation Initiated Early in Post-Stroke Recovery: A Feasibility Study.
Background: Enhanced neural plasticity early after stroke suggests the potential to improve outcomes with intensive rehabilitation therapy. Most patients do not get such therapy, however, due to limited access, changing rehabilitation therapy settings, low therapy doses, and poor compliance.
Objective: To examine the feasibility, safety, and potential efficacy of an established telerehabilitation (TR) program after stroke initiated during admission to an inpatient rehabilitation facility (IRF) and completed in the patient's home.
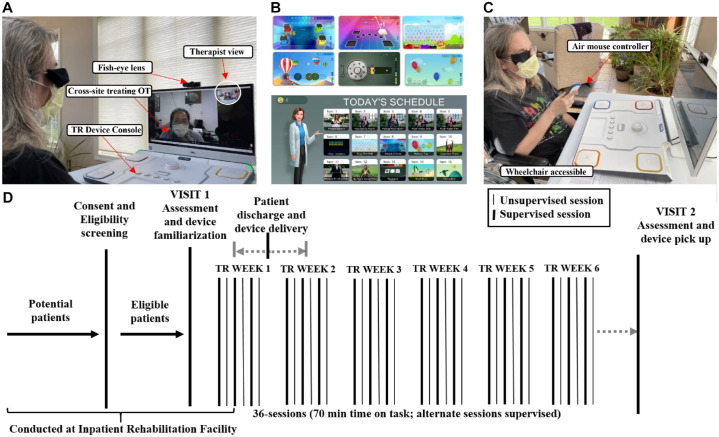
Methods: Participants with hemiparetic stroke admitted to an IRF received daily TR targeting arm motor function in addition to usual care. Treatment consisted of 36, 70-minute sessions (half supervised by a licensed therapist via videoconference), over a 6-week period, that included functional games, exercise videos, education, and daily assessments.
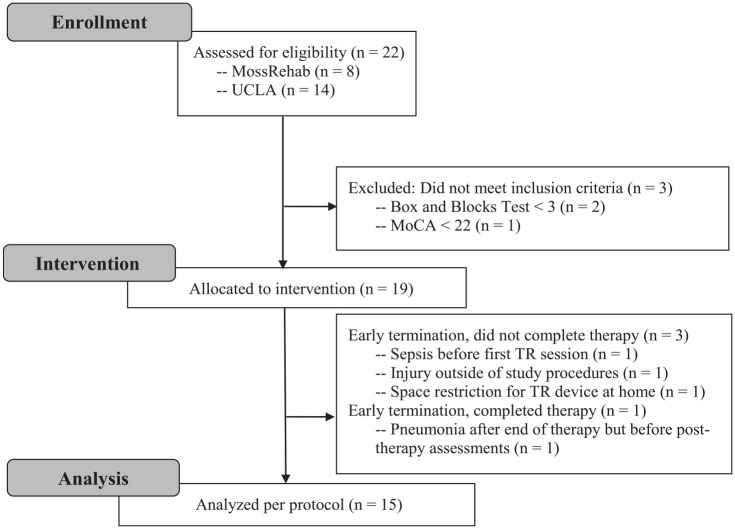
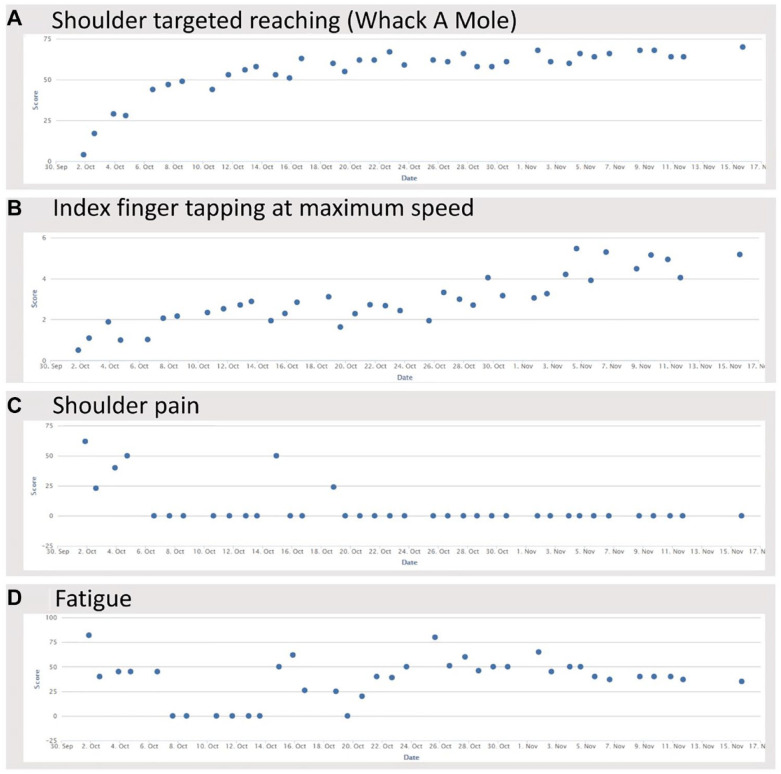
Results: Sixteen participants of 19 allocated completed the intervention (age 61.3 ± 9.4 years; 6 female; baseline Upper Extremity Fugl-Meyer [UEFM] score 35.9 ± 6.4 points, mean ± SD; NIHSS score 4 (3.75, 5.25), median, IQR; intervention commenced 28.3 ± 13.0 days post-stroke). Compliance was 100%, retention 84%, and patient satisfaction 93%; 2 patients developed COVID-19 and continued TR. Post-intervention UEFM improvement was 18.1 ± 10.9 points (P < .0001); Box and Blocks, 22.4 ± 9.8 blocks (P = .0001). Digital motor assessments, acquired daily in the home, were concordant with these gains. The dose of rehabilitation therapy received as usual care during this 6-week interval was 33.9 ± 20.3 hours; adding TR more than doubled this to 73.6 ± 21.8 hours (P < .0001). Patients enrolled in Philadelphia could be treated remotely by therapists in Los Angeles.
Conclusions: These results support feasibility, safety, and potential efficacy of providing intense TR therapy early after stroke.
期刊介绍:
Neurorehabilitation & Neural Repair (NNR) offers innovative and reliable reports relevant to functional recovery from neural injury and long term neurologic care. The journal''s unique focus is evidence-based basic and clinical practice and research. NNR deals with the management and fundamental mechanisms of functional recovery from conditions such as stroke, multiple sclerosis, Alzheimer''s disease, brain and spinal cord injuries, and peripheral nerve injuries.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
