Muhammed Ahmed Elhadedy, Ghada El-Kannishy, Ayman F Refaie, Hussein A Sheashaa, Ahmed Halawa
{"title":"肾移植前继发性甲状旁腺功能亢进的治疗:甲状旁腺切除术与甲状旁腺切除术。","authors":"Muhammed Ahmed Elhadedy, Ghada El-Kannishy, Ayman F Refaie, Hussein A Sheashaa, Ahmed Halawa","doi":"10.7573/dic.2022-11-5","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Secondary hyperparathyroidism is a common consequence of end-stage renal disease. Despite the efficacy of kidney transplantation in treating renal failure, many transplant recipients still suffer from persistent or tertiary hyperparathyroidism. Furthermore, the impact of secondary hyperparathyroidism therapy choices on other renal transplant outcomes is poorly understood.</p><p><strong>Methods: </strong>We retrieved the clinical data of 334 patients who received a kidney allograft between January 2007 and December 2014 at the Sheffield Teaching Hospitals, NHS Foundation Trust, United Kingdom. We identified three groups: parathyroidectomy group (34 patients), including patients who had parathyroidectomy before transplantation; cinacalcet group (31 patients), including patients who received cinacalcet before transplantation; and control group (269 patients), including patients who receive a transplant in the same period but did not have any evidence of hyperparathyroidism. We reviewed the demographic data, biochemical parameters and graft survival of all groups.</p><p><strong>Results: </strong>Patients who underwent parathyroidectomy before transplantation had significantly better post-transplant calcium and parathyroid hormone levels than patients in the cinacalcet group (<i>p</i>=0.003). In addition, a significantly lower number of patients had tertiary hyperparathyroidism in the parathyroidectomy group than in the cinacalcet group at 1 year of follow-up (<i>p</i>=0.001). However, short-term and long-term graft survival was comparable in all groups.</p><p><strong>Conclusions: </strong>Renal allograft survival was comparable in all groups. However, tertiary hyperparathyroidism was less likely to occur in patients who underwent parathyroidectomy than in those who were administered cinacalcet.</p>","PeriodicalId":11362,"journal":{"name":"Drugs in Context","volume":"12 ","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/49/be/dic-2022-11-5.PMC10108670.pdf","citationCount":"0","resultStr":"{\"title\":\"Management of pre-renal transplant secondary hyperparathyroidism: parathyroidectomy versus cinacalcet.\",\"authors\":\"Muhammed Ahmed Elhadedy, Ghada El-Kannishy, Ayman F Refaie, Hussein A Sheashaa, Ahmed Halawa\",\"doi\":\"10.7573/dic.2022-11-5\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Secondary hyperparathyroidism is a common consequence of end-stage renal disease. Despite the efficacy of kidney transplantation in treating renal failure, many transplant recipients still suffer from persistent or tertiary hyperparathyroidism. Furthermore, the impact of secondary hyperparathyroidism therapy choices on other renal transplant outcomes is poorly understood.</p><p><strong>Methods: </strong>We retrieved the clinical data of 334 patients who received a kidney allograft between January 2007 and December 2014 at the Sheffield Teaching Hospitals, NHS Foundation Trust, United Kingdom. We identified three groups: parathyroidectomy group (34 patients), including patients who had parathyroidectomy before transplantation; cinacalcet group (31 patients), including patients who received cinacalcet before transplantation; and control group (269 patients), including patients who receive a transplant in the same period but did not have any evidence of hyperparathyroidism. We reviewed the demographic data, biochemical parameters and graft survival of all groups.</p><p><strong>Results: </strong>Patients who underwent parathyroidectomy before transplantation had significantly better post-transplant calcium and parathyroid hormone levels than patients in the cinacalcet group (<i>p</i>=0.003). In addition, a significantly lower number of patients had tertiary hyperparathyroidism in the parathyroidectomy group than in the cinacalcet group at 1 year of follow-up (<i>p</i>=0.001). However, short-term and long-term graft survival was comparable in all groups.</p><p><strong>Conclusions: </strong>Renal allograft survival was comparable in all groups. However, tertiary hyperparathyroidism was less likely to occur in patients who underwent parathyroidectomy than in those who were administered cinacalcet.</p>\",\"PeriodicalId\":11362,\"journal\":{\"name\":\"Drugs in Context\",\"volume\":\"12 \",\"pages\":\"\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/49/be/dic-2022-11-5.PMC10108670.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Drugs in Context\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.7573/dic.2022-11-5\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"Pharmacology, Toxicology and Pharmaceutics\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Drugs in Context","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.7573/dic.2022-11-5","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"Pharmacology, Toxicology and Pharmaceutics","Score":null,"Total":0}
Management of pre-renal transplant secondary hyperparathyroidism: parathyroidectomy versus cinacalcet.
Background: Secondary hyperparathyroidism is a common consequence of end-stage renal disease. Despite the efficacy of kidney transplantation in treating renal failure, many transplant recipients still suffer from persistent or tertiary hyperparathyroidism. Furthermore, the impact of secondary hyperparathyroidism therapy choices on other renal transplant outcomes is poorly understood.
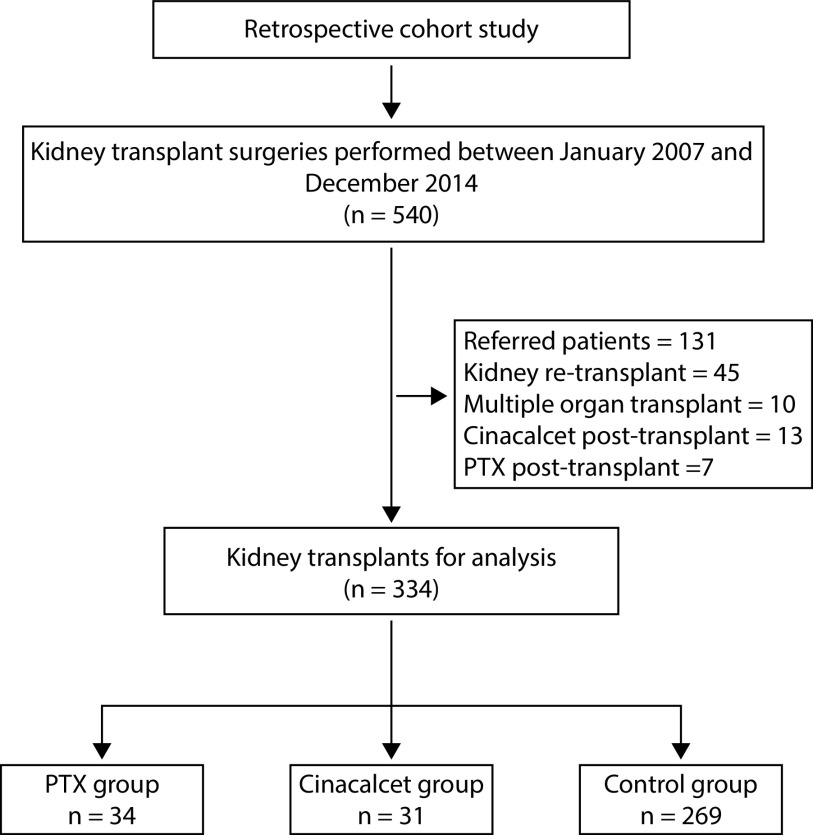
Methods: We retrieved the clinical data of 334 patients who received a kidney allograft between January 2007 and December 2014 at the Sheffield Teaching Hospitals, NHS Foundation Trust, United Kingdom. We identified three groups: parathyroidectomy group (34 patients), including patients who had parathyroidectomy before transplantation; cinacalcet group (31 patients), including patients who received cinacalcet before transplantation; and control group (269 patients), including patients who receive a transplant in the same period but did not have any evidence of hyperparathyroidism. We reviewed the demographic data, biochemical parameters and graft survival of all groups.
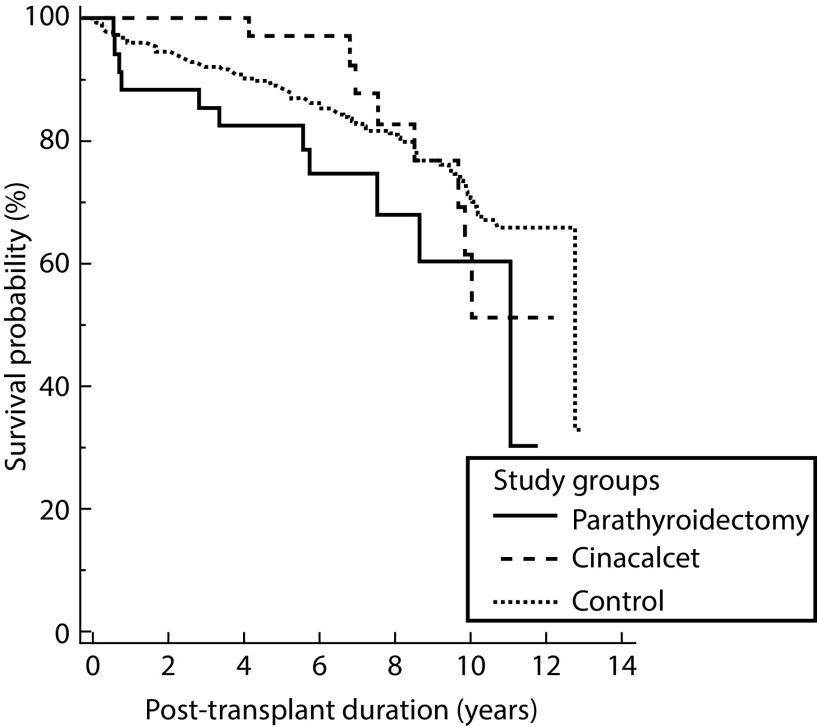
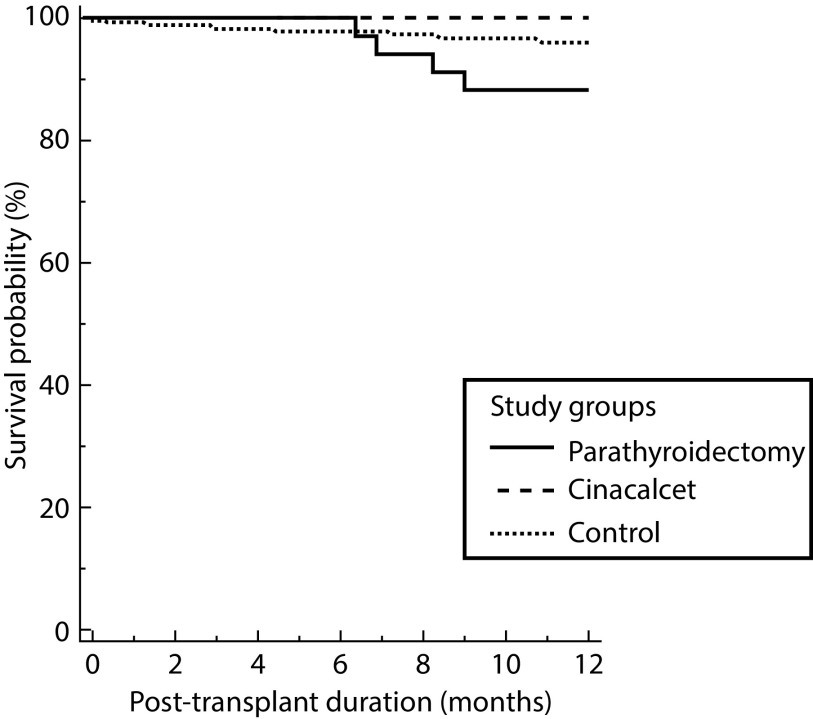
Results: Patients who underwent parathyroidectomy before transplantation had significantly better post-transplant calcium and parathyroid hormone levels than patients in the cinacalcet group (p=0.003). In addition, a significantly lower number of patients had tertiary hyperparathyroidism in the parathyroidectomy group than in the cinacalcet group at 1 year of follow-up (p=0.001). However, short-term and long-term graft survival was comparable in all groups.
Conclusions: Renal allograft survival was comparable in all groups. However, tertiary hyperparathyroidism was less likely to occur in patients who underwent parathyroidectomy than in those who were administered cinacalcet.
期刊介绍:
Covers all phases of original research: laboratory, animal and human/clinical studies, health economics and outcomes research, and postmarketing studies. Original research that shows positive or negative results are welcomed. Invited review articles may cover single-drug reviews, drug class reviews, latest advances in drug therapy, therapeutic-area reviews, place-in-therapy reviews, new pathways and classes of drugs. In addition, systematic reviews and meta-analyses are welcomed and may be published as original research if performed per accepted guidelines. Editorials of key topics and issues in drugs and therapeutics are welcomed. The Editor-in-Chief will also consider manuscripts of interest in areas such as technologies that support diagnosis, assessment and treatment. EQUATOR Network reporting guidelines should be followed for each article type. GPP3 Guidelines should be followed for any industry-sponsored manuscripts. Other Editorial sections may include Editorial, Case Report, Conference Report, Letter-to-the-Editor, Educational Section.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
