Reşit Yıldırım, Mustafa Dinler, Ahmet Özer, Nazife Şule Yaşar Bilge, Timuçin Kaşifoğlu
{"title":"家族性地中海热患者的霜状支血管炎诊断。","authors":"Reşit Yıldırım, Mustafa Dinler, Ahmet Özer, Nazife Şule Yaşar Bilge, Timuçin Kaşifoğlu","doi":"10.5152/eurjrheum.2022.22018","DOIUrl":null,"url":null,"abstract":"Corresponding author: Reşit Yıldırım E-mail: celeng18@gmail.com Received: March 18, 2022 Accepted: June 8, 2022 Publication Date: July 29, 2022 A 41-year-old female with a previous diagnosis of familial Mediterranean fever (FMF) was admitted due to a sudden-onset vision loss in the right eye during the third day of FMF attack. Past medical records revealed that she was non-compliant with her colchicine medication and therefore experienced 4 serositis attacks in the last 6 months. The systemic rheumatologic questionnaire was otherwise non-contributory. Ophthalmologic examination of the left eye demonstrated no pathology, whereas fundus evaluation of the right eye showed severe, white vascular sheaths extending from the optic disc to the periphery and preand intra-retinal hemorrhages in all retinal quadrants (Figure 1). Dilated and tortuous veins were detected in fluorescent angiography imaging (Figure 2). Based on these findings, a diagnosis of frosted branch angiitis (FBA) was made. Laboratory investigations were unremarkable except for mild elevations of acute phase parameters. Serologic studies for antinuclear antibody, anticardiolipin antibodies, and antineutrophil cytoplasmic antibodies (ANCA) were negative. Possible infectious agents were also excluded, and extensive radiographic evaluation of the central nervous system was non-revealing. After excluding all other possibilities, a diagnosis of FBA possibly related to FMF was considered and a combination of methylprednisolone (1 mg/kg/day) with tapering doses, azathioprine (2.5 mg/kg/day) and colchicine (0.5 mg, 3 times daily), was initiated. The visual complaints in the right eye completely resolved at the end of the third month. In the fourth month of follow-up, she manifested with sudden-onset vision loss in the same eye during a serositis attack. Colchicine dosage was escalated to 4 times a day with concomitant moderate steroid administration. She is currently on colchicine and azathioprine without any FMF attack and relapses of FBA in the last 6 months","PeriodicalId":12066,"journal":{"name":"European journal of rheumatology","volume":"10 1","pages":"47-48"},"PeriodicalIF":1.8000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/3c/be/ejr-10-1-47.PMC10152073.pdf","citationCount":"0","resultStr":"{\"title\":\"Frosted Branch Angiitis in a Patient with Familial Mediterranean Fever Diagnosis.\",\"authors\":\"Reşit Yıldırım, Mustafa Dinler, Ahmet Özer, Nazife Şule Yaşar Bilge, Timuçin Kaşifoğlu\",\"doi\":\"10.5152/eurjrheum.2022.22018\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"Corresponding author: Reşit Yıldırım E-mail: celeng18@gmail.com Received: March 18, 2022 Accepted: June 8, 2022 Publication Date: July 29, 2022 A 41-year-old female with a previous diagnosis of familial Mediterranean fever (FMF) was admitted due to a sudden-onset vision loss in the right eye during the third day of FMF attack. Past medical records revealed that she was non-compliant with her colchicine medication and therefore experienced 4 serositis attacks in the last 6 months. The systemic rheumatologic questionnaire was otherwise non-contributory. Ophthalmologic examination of the left eye demonstrated no pathology, whereas fundus evaluation of the right eye showed severe, white vascular sheaths extending from the optic disc to the periphery and preand intra-retinal hemorrhages in all retinal quadrants (Figure 1). Dilated and tortuous veins were detected in fluorescent angiography imaging (Figure 2). Based on these findings, a diagnosis of frosted branch angiitis (FBA) was made. Laboratory investigations were unremarkable except for mild elevations of acute phase parameters. Serologic studies for antinuclear antibody, anticardiolipin antibodies, and antineutrophil cytoplasmic antibodies (ANCA) were negative. Possible infectious agents were also excluded, and extensive radiographic evaluation of the central nervous system was non-revealing. After excluding all other possibilities, a diagnosis of FBA possibly related to FMF was considered and a combination of methylprednisolone (1 mg/kg/day) with tapering doses, azathioprine (2.5 mg/kg/day) and colchicine (0.5 mg, 3 times daily), was initiated. The visual complaints in the right eye completely resolved at the end of the third month. In the fourth month of follow-up, she manifested with sudden-onset vision loss in the same eye during a serositis attack. Colchicine dosage was escalated to 4 times a day with concomitant moderate steroid administration. She is currently on colchicine and azathioprine without any FMF attack and relapses of FBA in the last 6 months\",\"PeriodicalId\":12066,\"journal\":{\"name\":\"European journal of rheumatology\",\"volume\":\"10 1\",\"pages\":\"47-48\"},\"PeriodicalIF\":1.8000,\"publicationDate\":\"2023-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/3c/be/ejr-10-1-47.PMC10152073.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"European journal of rheumatology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.5152/eurjrheum.2022.22018\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q4\",\"JCRName\":\"RHEUMATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"European journal of rheumatology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5152/eurjrheum.2022.22018","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"RHEUMATOLOGY","Score":null,"Total":0}
Frosted Branch Angiitis in a Patient with Familial Mediterranean Fever Diagnosis.
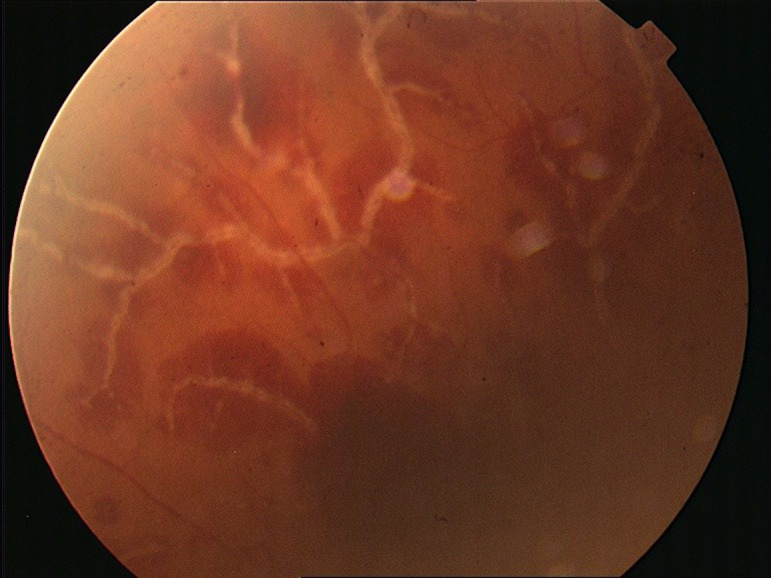
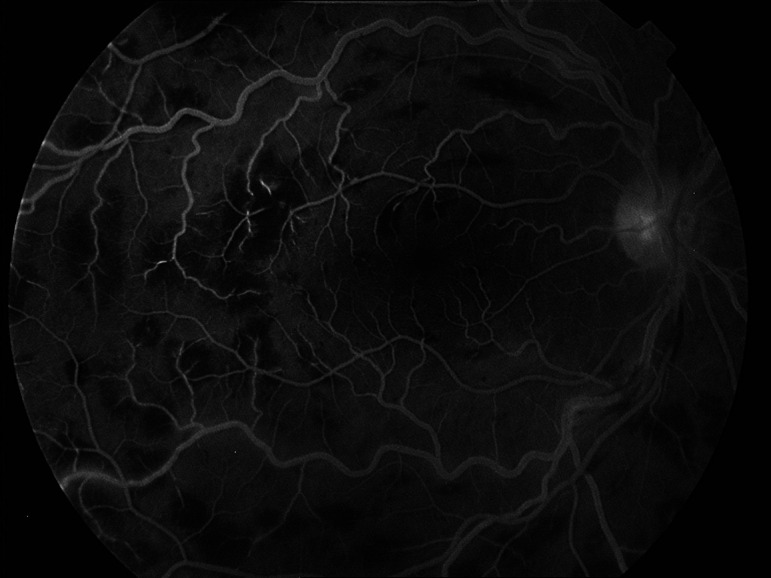
Corresponding author: Reşit Yıldırım E-mail: celeng18@gmail.com Received: March 18, 2022 Accepted: June 8, 2022 Publication Date: July 29, 2022 A 41-year-old female with a previous diagnosis of familial Mediterranean fever (FMF) was admitted due to a sudden-onset vision loss in the right eye during the third day of FMF attack. Past medical records revealed that she was non-compliant with her colchicine medication and therefore experienced 4 serositis attacks in the last 6 months. The systemic rheumatologic questionnaire was otherwise non-contributory. Ophthalmologic examination of the left eye demonstrated no pathology, whereas fundus evaluation of the right eye showed severe, white vascular sheaths extending from the optic disc to the periphery and preand intra-retinal hemorrhages in all retinal quadrants (Figure 1). Dilated and tortuous veins were detected in fluorescent angiography imaging (Figure 2). Based on these findings, a diagnosis of frosted branch angiitis (FBA) was made. Laboratory investigations were unremarkable except for mild elevations of acute phase parameters. Serologic studies for antinuclear antibody, anticardiolipin antibodies, and antineutrophil cytoplasmic antibodies (ANCA) were negative. Possible infectious agents were also excluded, and extensive radiographic evaluation of the central nervous system was non-revealing. After excluding all other possibilities, a diagnosis of FBA possibly related to FMF was considered and a combination of methylprednisolone (1 mg/kg/day) with tapering doses, azathioprine (2.5 mg/kg/day) and colchicine (0.5 mg, 3 times daily), was initiated. The visual complaints in the right eye completely resolved at the end of the third month. In the fourth month of follow-up, she manifested with sudden-onset vision loss in the same eye during a serositis attack. Colchicine dosage was escalated to 4 times a day with concomitant moderate steroid administration. She is currently on colchicine and azathioprine without any FMF attack and relapses of FBA in the last 6 months





 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
