{"title":"代谢综合征对高危酒精性肝炎患者预后的影响:重新定义酒精性肝炎。","authors":"Shahid Habib, Traci Murakami, Varun Takyar, Krunal Patel, Cristian Dominguez, Yongcheng Zhan, Omid Mehrpour, Chiu-Hsieh Hsu","doi":"10.14740/gr1556","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Alcoholic hepatitis (AH) is characterized by acute symptomatic hepatitis associated with heavy alcohol use. This study was designed to assess the impact of metabolic syndrome on high-risk patients with AH with discriminant function (DF) score ≥ 32 and its effect on mortality.</p><p><strong>Methods: </strong>We searched the hospital database for ICD-9 diagnosis codes of acute AH, alcoholic liver cirrhosis, and alcoholic liver damage. The entire cohort was categorized into two groups: AH and AH with metabolic syndrome. The effect of metabolic syndrome on mortality was evaluated. Also, an exploratory analysis was used to create a novel risk measure score to assess mortality.</p><p><strong>Results: </strong>A large proportion (75.5%) of the patients identified in the database who had been treated as AH had other etiologies and did not meet the American College of Gastroenterology (ACG)-defined diagnosis of acute AH, thus had been misdiagnosed as AH. Such patients were excluded from analysis. The mean body mass index (BMI), hemoglobin (Hb), hematocrit (HCT), and alcoholic liver disease/non-alcoholic fatty liver disease index (ANI) were significantly different between two groups (P < 0.05). The results of a univariate Cox regression model showed that age, BMI, white blood cells (WBCs), creatinine (Cr), international normalized ratio (INR), prothrombin time (PT), albumin levels, albumin < 3.5, total bilirubin, Na, Child-Turcotte-Pugh (CTP), model for end-stage liver disease (MELD), MELD ≥ 21, MELD ≥ 18, DF score, and DF ≥ 32 had a significant effect on mortality. Patients with a MELD greater than 21 had a hazard ratio (HR) (95% confidence interval (CI) of 5.81 (2.74 - 12.30) (P < 0.001). The adjusted Cox regression model results showed that age, Hb, Cr, INR, Na, MELD score, DF score, and metabolic syndrome were independently associated with high patient mortality. However, the increase in BMI and mean corpuscular volume (MCV) and sodium significantly reduced the risk of death. We found that a model including age, MELD ≥ 21, and albumin < 3.5 was the best model in identifying patient mortality. Our study showed that patients admitted with a diagnosis of alcoholic liver disease with metabolic syndrome had an increased mortality risk compared to patients without metabolic syndrome, in high-risk patients with DF ≥ 32 and MELD ≥ 21. A bivariate correlation analysis revealed that patients with AH with metabolic syndrome were more likely to have infection (43%) compared to AH (26%) with correlation coefficient of 0.176 (P = 0.03, CI: 0.018 - 1.0).</p><p><strong>Conclusion: </strong>In clinical practice, the diagnosis of AH is inaccurately applied. Metabolic syndrome significantly increases the mortality risk in high-risk AH. It signifies that the presence of features of metabolic syndrome modifies the behavior of AH in acute settings, warranting different therapeutic strategies. We propose that in defining AH, patients overlapping with metabolic syndrome may need to be excluded as their outcome is different with regard to risk of renal dysfunctions, infections and death.</p>","PeriodicalId":12461,"journal":{"name":"Gastroenterology Research","volume":"16 1","pages":"25-36"},"PeriodicalIF":1.7000,"publicationDate":"2023-02-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/1a/e0/gr-16-025.PMC9990531.pdf","citationCount":"0","resultStr":"{\"title\":\"The Impact of Metabolic Syndrome on the Prognosis of High-Risk Alcoholic Hepatitis Patients: Redefining Alcoholic Hepatitis.\",\"authors\":\"Shahid Habib, Traci Murakami, Varun Takyar, Krunal Patel, Cristian Dominguez, Yongcheng Zhan, Omid Mehrpour, Chiu-Hsieh Hsu\",\"doi\":\"10.14740/gr1556\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Alcoholic hepatitis (AH) is characterized by acute symptomatic hepatitis associated with heavy alcohol use. This study was designed to assess the impact of metabolic syndrome on high-risk patients with AH with discriminant function (DF) score ≥ 32 and its effect on mortality.</p><p><strong>Methods: </strong>We searched the hospital database for ICD-9 diagnosis codes of acute AH, alcoholic liver cirrhosis, and alcoholic liver damage. The entire cohort was categorized into two groups: AH and AH with metabolic syndrome. The effect of metabolic syndrome on mortality was evaluated. Also, an exploratory analysis was used to create a novel risk measure score to assess mortality.</p><p><strong>Results: </strong>A large proportion (75.5%) of the patients identified in the database who had been treated as AH had other etiologies and did not meet the American College of Gastroenterology (ACG)-defined diagnosis of acute AH, thus had been misdiagnosed as AH. Such patients were excluded from analysis. The mean body mass index (BMI), hemoglobin (Hb), hematocrit (HCT), and alcoholic liver disease/non-alcoholic fatty liver disease index (ANI) were significantly different between two groups (P < 0.05). The results of a univariate Cox regression model showed that age, BMI, white blood cells (WBCs), creatinine (Cr), international normalized ratio (INR), prothrombin time (PT), albumin levels, albumin < 3.5, total bilirubin, Na, Child-Turcotte-Pugh (CTP), model for end-stage liver disease (MELD), MELD ≥ 21, MELD ≥ 18, DF score, and DF ≥ 32 had a significant effect on mortality. Patients with a MELD greater than 21 had a hazard ratio (HR) (95% confidence interval (CI) of 5.81 (2.74 - 12.30) (P < 0.001). The adjusted Cox regression model results showed that age, Hb, Cr, INR, Na, MELD score, DF score, and metabolic syndrome were independently associated with high patient mortality. However, the increase in BMI and mean corpuscular volume (MCV) and sodium significantly reduced the risk of death. We found that a model including age, MELD ≥ 21, and albumin < 3.5 was the best model in identifying patient mortality. Our study showed that patients admitted with a diagnosis of alcoholic liver disease with metabolic syndrome had an increased mortality risk compared to patients without metabolic syndrome, in high-risk patients with DF ≥ 32 and MELD ≥ 21. A bivariate correlation analysis revealed that patients with AH with metabolic syndrome were more likely to have infection (43%) compared to AH (26%) with correlation coefficient of 0.176 (P = 0.03, CI: 0.018 - 1.0).</p><p><strong>Conclusion: </strong>In clinical practice, the diagnosis of AH is inaccurately applied. Metabolic syndrome significantly increases the mortality risk in high-risk AH. It signifies that the presence of features of metabolic syndrome modifies the behavior of AH in acute settings, warranting different therapeutic strategies. We propose that in defining AH, patients overlapping with metabolic syndrome may need to be excluded as their outcome is different with regard to risk of renal dysfunctions, infections and death.</p>\",\"PeriodicalId\":12461,\"journal\":{\"name\":\"Gastroenterology Research\",\"volume\":\"16 1\",\"pages\":\"25-36\"},\"PeriodicalIF\":1.7000,\"publicationDate\":\"2023-02-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/1a/e0/gr-16-025.PMC9990531.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Gastroenterology Research\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.14740/gr1556\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q4\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Gastroenterology Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14740/gr1556","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
The Impact of Metabolic Syndrome on the Prognosis of High-Risk Alcoholic Hepatitis Patients: Redefining Alcoholic Hepatitis.
Background: Alcoholic hepatitis (AH) is characterized by acute symptomatic hepatitis associated with heavy alcohol use. This study was designed to assess the impact of metabolic syndrome on high-risk patients with AH with discriminant function (DF) score ≥ 32 and its effect on mortality.
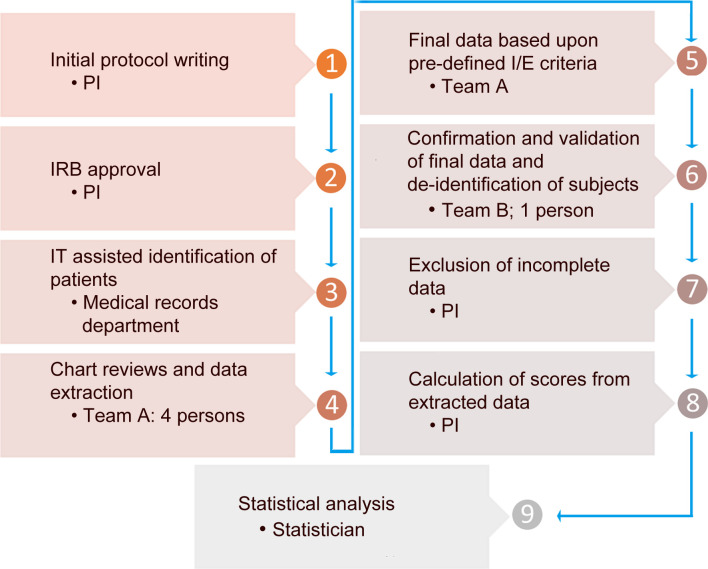
Methods: We searched the hospital database for ICD-9 diagnosis codes of acute AH, alcoholic liver cirrhosis, and alcoholic liver damage. The entire cohort was categorized into two groups: AH and AH with metabolic syndrome. The effect of metabolic syndrome on mortality was evaluated. Also, an exploratory analysis was used to create a novel risk measure score to assess mortality.
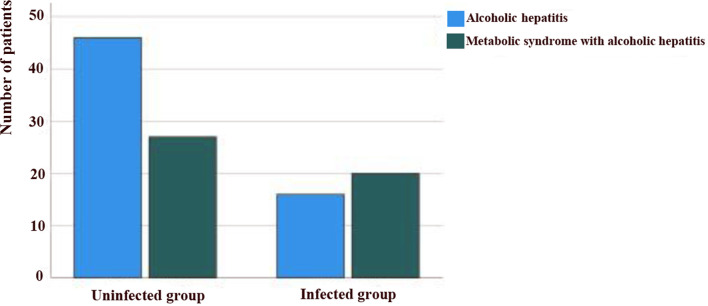
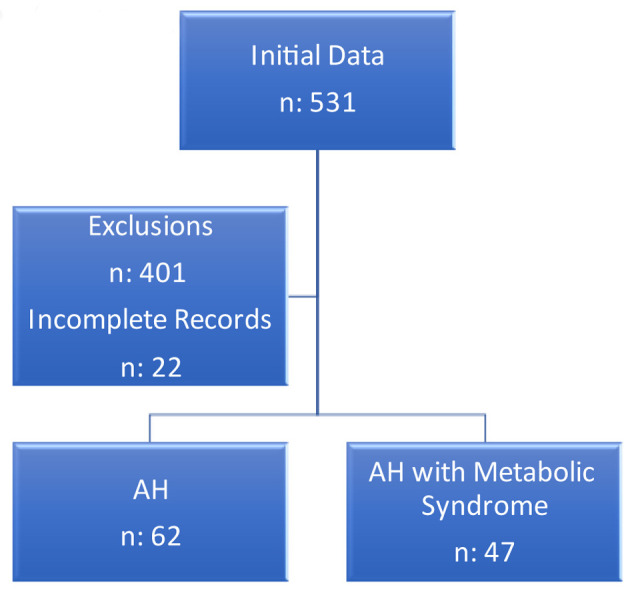
Results: A large proportion (75.5%) of the patients identified in the database who had been treated as AH had other etiologies and did not meet the American College of Gastroenterology (ACG)-defined diagnosis of acute AH, thus had been misdiagnosed as AH. Such patients were excluded from analysis. The mean body mass index (BMI), hemoglobin (Hb), hematocrit (HCT), and alcoholic liver disease/non-alcoholic fatty liver disease index (ANI) were significantly different between two groups (P < 0.05). The results of a univariate Cox regression model showed that age, BMI, white blood cells (WBCs), creatinine (Cr), international normalized ratio (INR), prothrombin time (PT), albumin levels, albumin < 3.5, total bilirubin, Na, Child-Turcotte-Pugh (CTP), model for end-stage liver disease (MELD), MELD ≥ 21, MELD ≥ 18, DF score, and DF ≥ 32 had a significant effect on mortality. Patients with a MELD greater than 21 had a hazard ratio (HR) (95% confidence interval (CI) of 5.81 (2.74 - 12.30) (P < 0.001). The adjusted Cox regression model results showed that age, Hb, Cr, INR, Na, MELD score, DF score, and metabolic syndrome were independently associated with high patient mortality. However, the increase in BMI and mean corpuscular volume (MCV) and sodium significantly reduced the risk of death. We found that a model including age, MELD ≥ 21, and albumin < 3.5 was the best model in identifying patient mortality. Our study showed that patients admitted with a diagnosis of alcoholic liver disease with metabolic syndrome had an increased mortality risk compared to patients without metabolic syndrome, in high-risk patients with DF ≥ 32 and MELD ≥ 21. A bivariate correlation analysis revealed that patients with AH with metabolic syndrome were more likely to have infection (43%) compared to AH (26%) with correlation coefficient of 0.176 (P = 0.03, CI: 0.018 - 1.0).
Conclusion: In clinical practice, the diagnosis of AH is inaccurately applied. Metabolic syndrome significantly increases the mortality risk in high-risk AH. It signifies that the presence of features of metabolic syndrome modifies the behavior of AH in acute settings, warranting different therapeutic strategies. We propose that in defining AH, patients overlapping with metabolic syndrome may need to be excluded as their outcome is different with regard to risk of renal dysfunctions, infections and death.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
