Sagar B. Dugani MD, PhD, MPH , Mohammad Zubaid MB ChB , Wafa Rashed MBBS , Marlene E. Girardo MS , Zuhur Balayah MSc , Samia Mora MD, MHS , Alawi A. Alsheikh-Ali MD, MSc
{"title":"过早和非过早急性冠状动脉综合征后健康和死亡率的社会决定因素","authors":"Sagar B. Dugani MD, PhD, MPH , Mohammad Zubaid MB ChB , Wafa Rashed MBBS , Marlene E. Girardo MS , Zuhur Balayah MSc , Samia Mora MD, MHS , Alawi A. Alsheikh-Ali MD, MSc","doi":"10.1016/j.mayocpiqo.2023.03.002","DOIUrl":null,"url":null,"abstract":"<div><h3>Objective</h3><p>To describe and compare the determinants of 1-year mortality after premature vs non-premature acute coronary syndrome (ACS).</p></div><div><h3>Patients and Methods</h3><p>Participants presenting with ACS were enrolled in a prospective registry of 29 hospitals in 4 countries, from January 22, 2012 to January 22, 2013, with 1-year of follow-up data. The primary outcome was all-cause 1-year mortality after premature ACS (men aged <55 years and women aged <65 years) and non-premature ACS (men aged ≥55 years and women aged ≥65 years). The associations between the baseline patient characteristics and 1-year mortality were analyzed in models adjusting for the Global Registry of Acute Coronary Events (GRACE) score and reported as adjusted odds ratio (aOR) (95% CI).</p></div><div><h3>Results</h3><p>Of the 3868 patients, 43.3% presented with premature ACS that was associated with lower 1-year mortality (5.7%) than those with non-premature ACS. In adjusted models, women experienced higher mortality than men after premature (aOR, 2.14 [1.37-3.41]) vs non-premature ACS (aOR, 1.28 [0.99-1.65]) (<em>P</em><sub>interaction</sub>=.047). Patients lacking formal education vs any education had higher mortality after both premature (aOR, 2.92 [1.87-4.61]) and non-premature ACS (aOR, 1.78 [1.36-2.34]) (<em>P</em><sub>interaction</sub>=.06). Lack of employment vs any employment was associated with approximately 3-fold higher mortality after premature and non-premature ACS (<em>P</em><sub>interaction</sub>=.72). Using stepwise logistic regression to predict 1-year mortality, a model with GRACE risk score and 4 characteristics (education, employment, body mass index [kg/m<sup>2</sup>], and statin use within 24 hours after admission) had higher discrimination than the GRACE risk score alone (area under the curve, 0.800 vs 0.773; <em>P</em><sub>comparison</sub>=.003).</p></div><div><h3>Conclusion</h3><p>In this study, women, compared with men, had higher 1-year mortality after premature ACS. The social determinants of health (no formal education or employment) were strongly associated with higher 1-year mortality after premature and non-premature ACS, improved mortality prediction, and should be routinely considered in risk assessment after ACS.</p></div>","PeriodicalId":94132,"journal":{"name":"Mayo Clinic proceedings. Innovations, quality & outcomes","volume":"7 3","pages":"Pages 153-164"},"PeriodicalIF":0.0000,"publicationDate":"2023-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/a2/32/main.PMC10160579.pdf","citationCount":"0","resultStr":"{\"title\":\"Social Determinants of Health and Mortality After Premature and Non-premature Acute Coronary Syndrome\",\"authors\":\"Sagar B. Dugani MD, PhD, MPH , Mohammad Zubaid MB ChB , Wafa Rashed MBBS , Marlene E. Girardo MS , Zuhur Balayah MSc , Samia Mora MD, MHS , Alawi A. Alsheikh-Ali MD, MSc\",\"doi\":\"10.1016/j.mayocpiqo.2023.03.002\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div><h3>Objective</h3><p>To describe and compare the determinants of 1-year mortality after premature vs non-premature acute coronary syndrome (ACS).</p></div><div><h3>Patients and Methods</h3><p>Participants presenting with ACS were enrolled in a prospective registry of 29 hospitals in 4 countries, from January 22, 2012 to January 22, 2013, with 1-year of follow-up data. The primary outcome was all-cause 1-year mortality after premature ACS (men aged <55 years and women aged <65 years) and non-premature ACS (men aged ≥55 years and women aged ≥65 years). The associations between the baseline patient characteristics and 1-year mortality were analyzed in models adjusting for the Global Registry of Acute Coronary Events (GRACE) score and reported as adjusted odds ratio (aOR) (95% CI).</p></div><div><h3>Results</h3><p>Of the 3868 patients, 43.3% presented with premature ACS that was associated with lower 1-year mortality (5.7%) than those with non-premature ACS. In adjusted models, women experienced higher mortality than men after premature (aOR, 2.14 [1.37-3.41]) vs non-premature ACS (aOR, 1.28 [0.99-1.65]) (<em>P</em><sub>interaction</sub>=.047). Patients lacking formal education vs any education had higher mortality after both premature (aOR, 2.92 [1.87-4.61]) and non-premature ACS (aOR, 1.78 [1.36-2.34]) (<em>P</em><sub>interaction</sub>=.06). Lack of employment vs any employment was associated with approximately 3-fold higher mortality after premature and non-premature ACS (<em>P</em><sub>interaction</sub>=.72). Using stepwise logistic regression to predict 1-year mortality, a model with GRACE risk score and 4 characteristics (education, employment, body mass index [kg/m<sup>2</sup>], and statin use within 24 hours after admission) had higher discrimination than the GRACE risk score alone (area under the curve, 0.800 vs 0.773; <em>P</em><sub>comparison</sub>=.003).</p></div><div><h3>Conclusion</h3><p>In this study, women, compared with men, had higher 1-year mortality after premature ACS. The social determinants of health (no formal education or employment) were strongly associated with higher 1-year mortality after premature and non-premature ACS, improved mortality prediction, and should be routinely considered in risk assessment after ACS.</p></div>\",\"PeriodicalId\":94132,\"journal\":{\"name\":\"Mayo Clinic proceedings. Innovations, quality & outcomes\",\"volume\":\"7 3\",\"pages\":\"Pages 153-164\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-06-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/a2/32/main.PMC10160579.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Mayo Clinic proceedings. Innovations, quality & outcomes\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://www.sciencedirect.com/science/article/pii/S2542454823000127\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/4/22 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Mayo Clinic proceedings. Innovations, quality & outcomes","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2542454823000127","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/4/22 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
Social Determinants of Health and Mortality After Premature and Non-premature Acute Coronary Syndrome
Objective
To describe and compare the determinants of 1-year mortality after premature vs non-premature acute coronary syndrome (ACS).
Patients and Methods
Participants presenting with ACS were enrolled in a prospective registry of 29 hospitals in 4 countries, from January 22, 2012 to January 22, 2013, with 1-year of follow-up data. The primary outcome was all-cause 1-year mortality after premature ACS (men aged <55 years and women aged <65 years) and non-premature ACS (men aged ≥55 years and women aged ≥65 years). The associations between the baseline patient characteristics and 1-year mortality were analyzed in models adjusting for the Global Registry of Acute Coronary Events (GRACE) score and reported as adjusted odds ratio (aOR) (95% CI).
Results
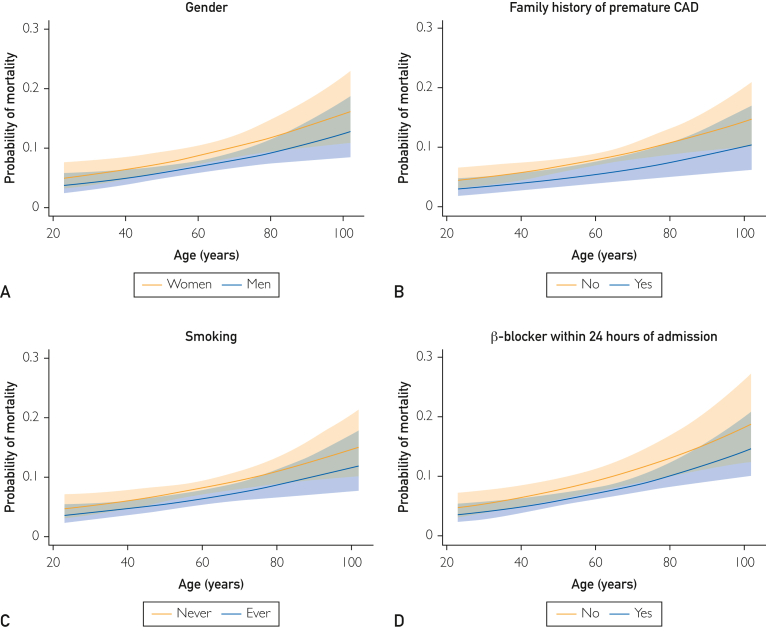
Of the 3868 patients, 43.3% presented with premature ACS that was associated with lower 1-year mortality (5.7%) than those with non-premature ACS. In adjusted models, women experienced higher mortality than men after premature (aOR, 2.14 [1.37-3.41]) vs non-premature ACS (aOR, 1.28 [0.99-1.65]) (Pinteraction=.047). Patients lacking formal education vs any education had higher mortality after both premature (aOR, 2.92 [1.87-4.61]) and non-premature ACS (aOR, 1.78 [1.36-2.34]) (Pinteraction=.06). Lack of employment vs any employment was associated with approximately 3-fold higher mortality after premature and non-premature ACS (Pinteraction=.72). Using stepwise logistic regression to predict 1-year mortality, a model with GRACE risk score and 4 characteristics (education, employment, body mass index [kg/m2], and statin use within 24 hours after admission) had higher discrimination than the GRACE risk score alone (area under the curve, 0.800 vs 0.773; Pcomparison=.003).
Conclusion
In this study, women, compared with men, had higher 1-year mortality after premature ACS. The social determinants of health (no formal education or employment) were strongly associated with higher 1-year mortality after premature and non-premature ACS, improved mortality prediction, and should be routinely considered in risk assessment after ACS.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
