Michel Oskam, Richard C van Kleef, René C J A van Vliet
{"title":"改进诊断为基础的成本组在荷兰风险均衡模型:一种新的聚类方法的影响,并允许多病。","authors":"Michel Oskam, Richard C van Kleef, René C J A van Vliet","doi":"10.1007/s10754-023-09345-0","DOIUrl":null,"url":null,"abstract":"<p><p>Health insurance markets with community-rated premiums typically use risk equalization (RE) to compensate insurers for predictable profits on people in good health and predictable losses on those with a chronic disease. Over the past decades RE models have evolved from simple demographic models to sophisticated health-based models. Despite the improvements, however, non-trivial predictable profits and losses remain. This study examines to what extent the Dutch RE model can be further improved by redesigning one key morbidity adjuster: the Diagnosis-based Cost Groups (DCGs). This redesign includes (1) revision of the underlying hospital diagnoses and treatments ('dxgroups'), (2) application of a new clustering procedure, and (3) allowing multi-qualification. We combine data on spending, risk characteristics and hospital claims for all individuals with basic health insurance in the Netherlands in 2017 (N = 17 m) with morbidity data from general practitioners (GPs) for a subsample (N = 1.3 m). We first simulate a baseline RE model (i.e., the RE model of 2020) and then modify three important features of the DCGs. In a second step, we evaluate the effect of the modifications in terms of predictable profits and losses for subgroups of consumers that are potentially vulnerable to risk selection. While less prominent results are found for subgroups derived from the GP data, our results demonstrate substantial reductions in predictable profits and losses at the level of dxgroups and for individuals with multiple dxgroups. An important takeaway from our paper is that smart design of morbidity adjusters in RE can help mitigate selection incentives.</p>","PeriodicalId":44403,"journal":{"name":"International Journal of Health Economics and Management","volume":"23 2","pages":"303-324"},"PeriodicalIF":1.5000,"publicationDate":"2023-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10156830/pdf/","citationCount":"1","resultStr":"{\"title\":\"Improving diagnosis-based cost groups in the Dutch risk equalization model: the effects of a new clustering method and allowing for multimorbidity.\",\"authors\":\"Michel Oskam, Richard C van Kleef, René C J A van Vliet\",\"doi\":\"10.1007/s10754-023-09345-0\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Health insurance markets with community-rated premiums typically use risk equalization (RE) to compensate insurers for predictable profits on people in good health and predictable losses on those with a chronic disease. Over the past decades RE models have evolved from simple demographic models to sophisticated health-based models. Despite the improvements, however, non-trivial predictable profits and losses remain. This study examines to what extent the Dutch RE model can be further improved by redesigning one key morbidity adjuster: the Diagnosis-based Cost Groups (DCGs). This redesign includes (1) revision of the underlying hospital diagnoses and treatments ('dxgroups'), (2) application of a new clustering procedure, and (3) allowing multi-qualification. We combine data on spending, risk characteristics and hospital claims for all individuals with basic health insurance in the Netherlands in 2017 (N = 17 m) with morbidity data from general practitioners (GPs) for a subsample (N = 1.3 m). We first simulate a baseline RE model (i.e., the RE model of 2020) and then modify three important features of the DCGs. In a second step, we evaluate the effect of the modifications in terms of predictable profits and losses for subgroups of consumers that are potentially vulnerable to risk selection. While less prominent results are found for subgroups derived from the GP data, our results demonstrate substantial reductions in predictable profits and losses at the level of dxgroups and for individuals with multiple dxgroups. An important takeaway from our paper is that smart design of morbidity adjusters in RE can help mitigate selection incentives.</p>\",\"PeriodicalId\":44403,\"journal\":{\"name\":\"International Journal of Health Economics and Management\",\"volume\":\"23 2\",\"pages\":\"303-324\"},\"PeriodicalIF\":1.5000,\"publicationDate\":\"2023-06-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10156830/pdf/\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"International Journal of Health Economics and Management\",\"FirstCategoryId\":\"96\",\"ListUrlMain\":\"https://doi.org/10.1007/s10754-023-09345-0\",\"RegionNum\":4,\"RegionCategory\":\"经济学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"BUSINESS, FINANCE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Journal of Health Economics and Management","FirstCategoryId":"96","ListUrlMain":"https://doi.org/10.1007/s10754-023-09345-0","RegionNum":4,"RegionCategory":"经济学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"BUSINESS, FINANCE","Score":null,"Total":0}
Improving diagnosis-based cost groups in the Dutch risk equalization model: the effects of a new clustering method and allowing for multimorbidity.
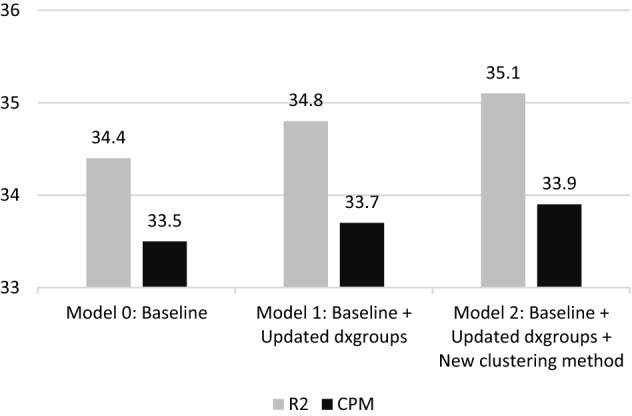
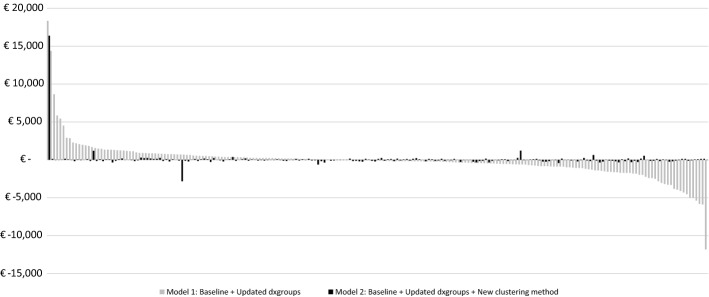
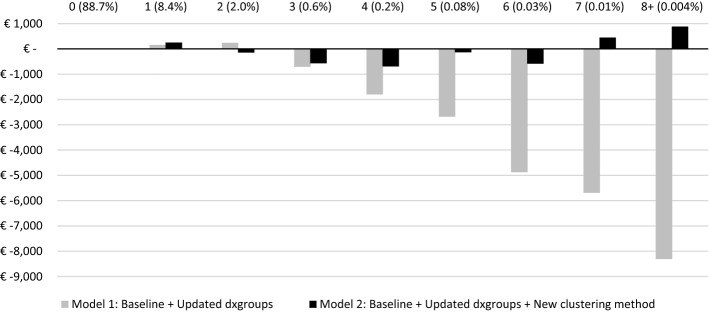
Health insurance markets with community-rated premiums typically use risk equalization (RE) to compensate insurers for predictable profits on people in good health and predictable losses on those with a chronic disease. Over the past decades RE models have evolved from simple demographic models to sophisticated health-based models. Despite the improvements, however, non-trivial predictable profits and losses remain. This study examines to what extent the Dutch RE model can be further improved by redesigning one key morbidity adjuster: the Diagnosis-based Cost Groups (DCGs). This redesign includes (1) revision of the underlying hospital diagnoses and treatments ('dxgroups'), (2) application of a new clustering procedure, and (3) allowing multi-qualification. We combine data on spending, risk characteristics and hospital claims for all individuals with basic health insurance in the Netherlands in 2017 (N = 17 m) with morbidity data from general practitioners (GPs) for a subsample (N = 1.3 m). We first simulate a baseline RE model (i.e., the RE model of 2020) and then modify three important features of the DCGs. In a second step, we evaluate the effect of the modifications in terms of predictable profits and losses for subgroups of consumers that are potentially vulnerable to risk selection. While less prominent results are found for subgroups derived from the GP data, our results demonstrate substantial reductions in predictable profits and losses at the level of dxgroups and for individuals with multiple dxgroups. An important takeaway from our paper is that smart design of morbidity adjusters in RE can help mitigate selection incentives.
期刊介绍:
The focus of the International Journal of Health Economics and Management is on health care systems and on the behavior of consumers, patients, and providers of such services. The links among management, public policy, payment, and performance are core topics of the relaunched journal. The demand for health care and its cost remain central concerns. Even as medical innovation allows providers to improve the lives of their patients, questions remain about how to efficiently deliver health care services, how to pay for it, and who should pay for it. These are central questions facing innovators, providers, and payers in the public and private sectors. One key to answering these questions is to understand how people choose among alternative arrangements, either in markets or through the political process. The choices made by healthcare managers concerning the organization and production of that care are also crucial. There is an important connection between the management of a health care system and its economic performance. The primary audience for this journal will be health economists and researchers in health management, along with the larger group of health services researchers. In addition, research and policy analysis reported in the journal should be of interest to health care providers, managers and policymakers, who need to know about the pressures facing insurers and governments, with consequences for regulation and mandates. The editors of the journal encourage submissions that analyze the behavior and interaction of the actors in health care, viz. consumers, providers, insurers, and governments. Preference will be given to contributions that combine theoretical with empirical work, evaluate conflicting findings, present new information, or compare experiences between countries and jurisdictions. In addition to conventional research articles, the journal will include specific subsections for shorter concise research findings and cont ributions to management and policy that provide important descriptive data or arguments about what policies follow from research findings. The composition of the editorial board is designed to cover the range of interest among economics and management researchers.Officially cited as: Int J Health Econ ManagFrom 2001 to 2014 the journal was published as International Journal of Health Care Finance and Economics. (Articles published in Vol. 1-14 officially cited as: Int J Health Care Finance Econ)


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
