Paula Hofstetter, Hanna Schröder, Stefan K Beckers, Christina Borgs, Rolf Rossaint, Marc Felzen
{"title":"紧急医疗服务中的固定-是否考虑了CSR和nexus标准?现场急救医师与远程急救医师治疗创伤患者的配对分析。","authors":"Paula Hofstetter, Hanna Schröder, Stefan K Beckers, Christina Borgs, Rolf Rossaint, Marc Felzen","doi":"10.2147/OAEM.S386650","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The NEXUS-low-risk criteria (NEXUS) and Canadian C-spine rule (CSR) are clinical decision tools used for the prehospital spinal clearance in trauma patients, intending to prevent over- as well as under immobilization. Since 2014, a holistic telemedicine system is part of the emergency medical service (EMS) in Aachen (Germany). This study aims to examine whether the decisions to immobilize or not by EMS- and tele-EMS physicians are based on NEXUS and the CSR, as well as the guideline adherence concerning the choice of immobilization device.</p><p><strong>Methods: </strong>A single-site retrospective chart review was undertaken. Inclusion criteria were EMS physician and tele-EMS physician protocols with traumatic diagnoses. Matched pairs were formed, using age, sex and working diagnoses as matching criteria. The primary outcome parameters were the criteria documented as well as the immobilization device used. The evaluation of the decision to immobilize based on the criteria documented was defined as secondary outcome parameter.</p><p><strong>Results: </strong>Of a total of 247 patients, 34% (n = 84) were immobilized in the EMS physician group and 32.79% (n = 81) in the tele-EMS physician group. In both groups, less than 7% NEXUS or CSR criteria were documented completely. The decision to immobilize or not was appropriately implemented in 127 (51%) in the EMS-physician and in 135 (54, 66%) in the tele-EMS physician group. Immobilization without indication was performed significantly more often by tele-EMS physicians (6.88% vs 2.02%). A significantly better guideline adherence was found in the tele-EMS physician group, preferring the vacuum mattress (25, 1% vs 8.9%) over the spineboard.</p><p><strong>Conclusion: </strong>It could be shown that NEXUS and CSR are not applied regularly, and if so, mostly inconsistently with incomplete documentation by both EMS- and tele-EMS physicians. Regarding the choice of the immobilization device a higher guideline adherence was shown among the tele-EMS physicians.</p>","PeriodicalId":74347,"journal":{"name":"","volume":"15 ","pages":"145-155"},"PeriodicalIF":0.0,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/0d/bc/oaem-15-145.PMC10178902.pdf","citationCount":"1","resultStr":"{\"title\":\"Immobilization in Emergency Medical Service - Are CSR and NEXUS-Criteria Considered? A Matched-Pairs Analysis Between Trauma Patients Treated by Onsite EMS Physicians and Patients Treated by Tele-EMS Physicians.\",\"authors\":\"Paula Hofstetter, Hanna Schröder, Stefan K Beckers, Christina Borgs, Rolf Rossaint, Marc Felzen\",\"doi\":\"10.2147/OAEM.S386650\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>The NEXUS-low-risk criteria (NEXUS) and Canadian C-spine rule (CSR) are clinical decision tools used for the prehospital spinal clearance in trauma patients, intending to prevent over- as well as under immobilization. Since 2014, a holistic telemedicine system is part of the emergency medical service (EMS) in Aachen (Germany). This study aims to examine whether the decisions to immobilize or not by EMS- and tele-EMS physicians are based on NEXUS and the CSR, as well as the guideline adherence concerning the choice of immobilization device.</p><p><strong>Methods: </strong>A single-site retrospective chart review was undertaken. Inclusion criteria were EMS physician and tele-EMS physician protocols with traumatic diagnoses. Matched pairs were formed, using age, sex and working diagnoses as matching criteria. The primary outcome parameters were the criteria documented as well as the immobilization device used. The evaluation of the decision to immobilize based on the criteria documented was defined as secondary outcome parameter.</p><p><strong>Results: </strong>Of a total of 247 patients, 34% (n = 84) were immobilized in the EMS physician group and 32.79% (n = 81) in the tele-EMS physician group. In both groups, less than 7% NEXUS or CSR criteria were documented completely. The decision to immobilize or not was appropriately implemented in 127 (51%) in the EMS-physician and in 135 (54, 66%) in the tele-EMS physician group. Immobilization without indication was performed significantly more often by tele-EMS physicians (6.88% vs 2.02%). A significantly better guideline adherence was found in the tele-EMS physician group, preferring the vacuum mattress (25, 1% vs 8.9%) over the spineboard.</p><p><strong>Conclusion: </strong>It could be shown that NEXUS and CSR are not applied regularly, and if so, mostly inconsistently with incomplete documentation by both EMS- and tele-EMS physicians. Regarding the choice of the immobilization device a higher guideline adherence was shown among the tele-EMS physicians.</p>\",\"PeriodicalId\":74347,\"journal\":{\"name\":\"\",\"volume\":\"15 \",\"pages\":\"145-155\"},\"PeriodicalIF\":0.0,\"publicationDate\":\"2023-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/0d/bc/oaem-15-145.PMC10178902.pdf\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.2147/OAEM.S386650\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/OAEM.S386650","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 1
摘要
背景:NEXUS-低风险标准(NEXUS)和加拿大颈椎规则(CSR)是用于创伤患者院前脊柱清除的临床决策工具,旨在防止过度和不固定。自2014年以来,整体远程医疗系统是亚琛(德国)紧急医疗服务(EMS)的一部分。本研究旨在探讨EMS医师和远程EMS医师是否基于NEXUS和CSR,以及关于固定装置选择的指南依从性来决定是否进行固定。方法:采用单点回顾性图表分析。纳入标准为创伤诊断的EMS医师和远程EMS医师协议。以年龄、性别和工作诊断作为匹配标准,形成配对组。主要结局参数是记录的标准以及使用的固定装置。根据所记录的标准评估是否进行固定被定义为次要结果参数。结果:247例患者中,EMS医师组有34% (n = 84)固定,远程EMS医师组有32.79% (n = 81)固定。在两组中,只有不到7%的NEXUS或CSR标准被完整记录。127名ems医生(51%)和135名远程ems医生(54.66%)正确地执行了固定或不固定的决定。无指征的固定术在远程ems医师中更为常见(6.88% vs 2.02%)。远程ems医师组的指南依从性明显更好,他们更喜欢真空床垫(25.1% vs 8.9%)而不是脊柱板。结论:可以表明NEXUS和CSR没有被定期应用,如果是的话,主要与EMS和远程EMS医生不完整的文件不一致。对于固定装置的选择,远程ems医师的指南依从性较高。
Immobilization in Emergency Medical Service - Are CSR and NEXUS-Criteria Considered? A Matched-Pairs Analysis Between Trauma Patients Treated by Onsite EMS Physicians and Patients Treated by Tele-EMS Physicians.
Background: The NEXUS-low-risk criteria (NEXUS) and Canadian C-spine rule (CSR) are clinical decision tools used for the prehospital spinal clearance in trauma patients, intending to prevent over- as well as under immobilization. Since 2014, a holistic telemedicine system is part of the emergency medical service (EMS) in Aachen (Germany). This study aims to examine whether the decisions to immobilize or not by EMS- and tele-EMS physicians are based on NEXUS and the CSR, as well as the guideline adherence concerning the choice of immobilization device.
Methods: A single-site retrospective chart review was undertaken. Inclusion criteria were EMS physician and tele-EMS physician protocols with traumatic diagnoses. Matched pairs were formed, using age, sex and working diagnoses as matching criteria. The primary outcome parameters were the criteria documented as well as the immobilization device used. The evaluation of the decision to immobilize based on the criteria documented was defined as secondary outcome parameter.
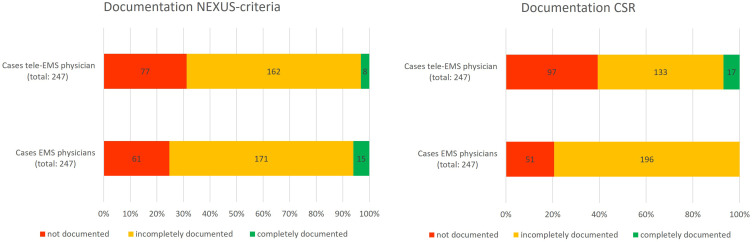
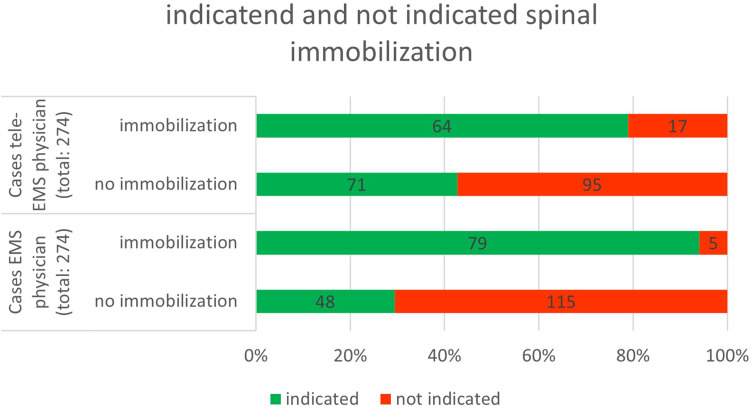
Results: Of a total of 247 patients, 34% (n = 84) were immobilized in the EMS physician group and 32.79% (n = 81) in the tele-EMS physician group. In both groups, less than 7% NEXUS or CSR criteria were documented completely. The decision to immobilize or not was appropriately implemented in 127 (51%) in the EMS-physician and in 135 (54, 66%) in the tele-EMS physician group. Immobilization without indication was performed significantly more often by tele-EMS physicians (6.88% vs 2.02%). A significantly better guideline adherence was found in the tele-EMS physician group, preferring the vacuum mattress (25, 1% vs 8.9%) over the spineboard.
Conclusion: It could be shown that NEXUS and CSR are not applied regularly, and if so, mostly inconsistently with incomplete documentation by both EMS- and tele-EMS physicians. Regarding the choice of the immobilization device a higher guideline adherence was shown among the tele-EMS physicians.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
