{"title":"危重病人根据肾功能不同,高蛋白供给对氮负荷有影响。","authors":"Masaki Mochizuki, Hidehiko Nakano, Daisuke Ikechi, Yuji Takahashi, Hideki Hashimoto, Kensuke Nakamura","doi":"10.3164/jcbn.22-87","DOIUrl":null,"url":null,"abstract":"<p><p>Adequate protein delivery is recommended in the acute phase of critical illness with kidney dysfunction. However, the influence of the protein and nitrogen loads has not yet been clarified. Patients admitted to the intensive care unit were included. In the former period, patients received standard care (0.9 g/kg/day protein). In the latter, patients received the intervention of active nutrition therapy with high protein delivery (1.8 g/kg/day protein). Fifty patients in the standard care group and 61 in the intervention group were examined. Maximum blood urea nitrogen (BUN) on days 7-10 were 27.9 (17.3, 38.6) vs 33 (26.3, 51.8) (mg/dl) (<i>p</i> = 0.031). The maximum difference in BUN increased [31.3 (22.8, 55) vs 50 (37.3, 75.9) mg/dl (<i>p</i> = 0.047)] when patients were limited to an estimated glomerular filtration rate (eGFR) <50 ml/min/1.73 m<sup>2</sup>. This difference increased further when patients were limited to eGFR <30 ml/min/1.73 m<sup>2</sup>. No significant differences were observed in maximum Cre or in the use of RRT. In conclusion, the provision of 1.8 g/kg/day protein was associated with an increase in BUN in critically ill patients with kidney dysfunction; however, it was tolerated without the need for RRT.</p>","PeriodicalId":15429,"journal":{"name":"Journal of Clinical Biochemistry and Nutrition","volume":"72 3","pages":"289-294"},"PeriodicalIF":1.7000,"publicationDate":"2023-05-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/11/3c/jcbn22-87.PMC10209593.pdf","citationCount":"0","resultStr":"{\"title\":\"The nitrogen load is affected by high protein provision according to kidney function in critically ill patients.\",\"authors\":\"Masaki Mochizuki, Hidehiko Nakano, Daisuke Ikechi, Yuji Takahashi, Hideki Hashimoto, Kensuke Nakamura\",\"doi\":\"10.3164/jcbn.22-87\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Adequate protein delivery is recommended in the acute phase of critical illness with kidney dysfunction. However, the influence of the protein and nitrogen loads has not yet been clarified. Patients admitted to the intensive care unit were included. In the former period, patients received standard care (0.9 g/kg/day protein). In the latter, patients received the intervention of active nutrition therapy with high protein delivery (1.8 g/kg/day protein). Fifty patients in the standard care group and 61 in the intervention group were examined. Maximum blood urea nitrogen (BUN) on days 7-10 were 27.9 (17.3, 38.6) vs 33 (26.3, 51.8) (mg/dl) (<i>p</i> = 0.031). The maximum difference in BUN increased [31.3 (22.8, 55) vs 50 (37.3, 75.9) mg/dl (<i>p</i> = 0.047)] when patients were limited to an estimated glomerular filtration rate (eGFR) <50 ml/min/1.73 m<sup>2</sup>. This difference increased further when patients were limited to eGFR <30 ml/min/1.73 m<sup>2</sup>. No significant differences were observed in maximum Cre or in the use of RRT. In conclusion, the provision of 1.8 g/kg/day protein was associated with an increase in BUN in critically ill patients with kidney dysfunction; however, it was tolerated without the need for RRT.</p>\",\"PeriodicalId\":15429,\"journal\":{\"name\":\"Journal of Clinical Biochemistry and Nutrition\",\"volume\":\"72 3\",\"pages\":\"289-294\"},\"PeriodicalIF\":1.7000,\"publicationDate\":\"2023-05-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/11/3c/jcbn22-87.PMC10209593.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Clinical Biochemistry and Nutrition\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.3164/jcbn.22-87\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"NUTRITION & DIETETICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Clinical Biochemistry and Nutrition","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.3164/jcbn.22-87","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"NUTRITION & DIETETICS","Score":null,"Total":0}
The nitrogen load is affected by high protein provision according to kidney function in critically ill patients.
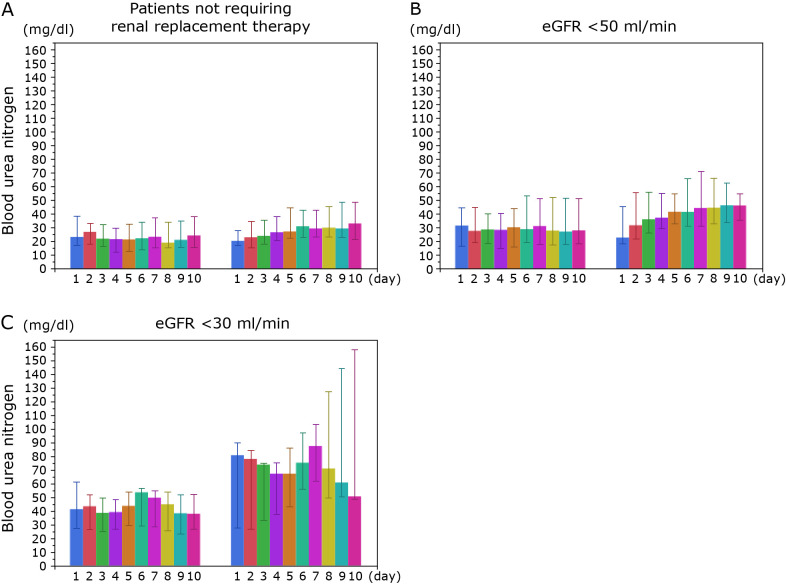
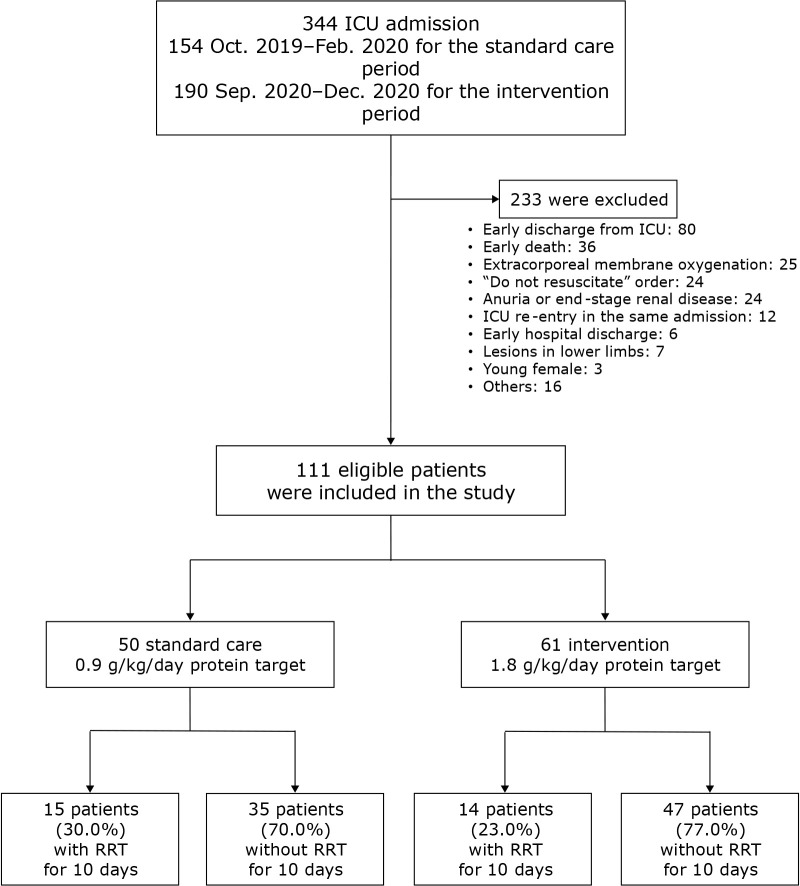
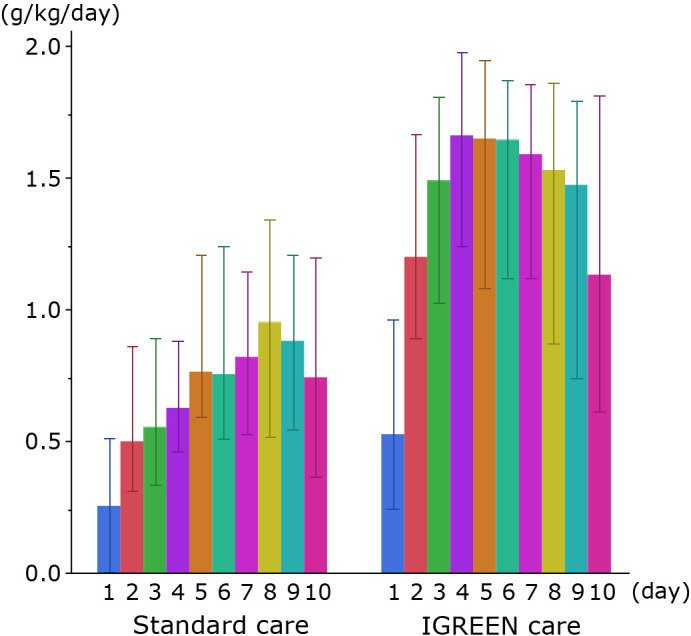
Adequate protein delivery is recommended in the acute phase of critical illness with kidney dysfunction. However, the influence of the protein and nitrogen loads has not yet been clarified. Patients admitted to the intensive care unit were included. In the former period, patients received standard care (0.9 g/kg/day protein). In the latter, patients received the intervention of active nutrition therapy with high protein delivery (1.8 g/kg/day protein). Fifty patients in the standard care group and 61 in the intervention group were examined. Maximum blood urea nitrogen (BUN) on days 7-10 were 27.9 (17.3, 38.6) vs 33 (26.3, 51.8) (mg/dl) (p = 0.031). The maximum difference in BUN increased [31.3 (22.8, 55) vs 50 (37.3, 75.9) mg/dl (p = 0.047)] when patients were limited to an estimated glomerular filtration rate (eGFR) <50 ml/min/1.73 m2. This difference increased further when patients were limited to eGFR <30 ml/min/1.73 m2. No significant differences were observed in maximum Cre or in the use of RRT. In conclusion, the provision of 1.8 g/kg/day protein was associated with an increase in BUN in critically ill patients with kidney dysfunction; however, it was tolerated without the need for RRT.
期刊介绍:
Journal of Clinical Biochemistry and Nutrition (JCBN) is
an international, interdisciplinary publication encompassing
chemical, biochemical, physiological, pathological, toxicological and medical approaches to research on lipid peroxidation, free radicals, oxidative stress and nutrition. The
Journal welcomes original contributions dealing with all
aspects of clinical biochemistry and clinical nutrition
including both in vitro and in vivo studies.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
