Seife Yohannes, Nitin Seam, Junfeng Sun, Joel McAlduff, Janet L Thorne, Susanne B Lara, Michael Keller
{"title":"SARS-COV2肺炎住院患者早期预警系统方案对ICU住院的影响","authors":"Seife Yohannes, Nitin Seam, Junfeng Sun, Joel McAlduff, Janet L Thorne, Susanne B Lara, Michael Keller","doi":"10.1177/11795484231156755","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>COVID-19 placed a significant burden on the global healthcare system. Strain in critical care capacity has been associated with increased COVID-19-related ICU mortality. This study evaluates the impact of an early warning system and response team implemented on medical floors to safely triage and care for critically ill patients on the floor and preserve ICU capacity.</p><p><strong>Methods: </strong>We conducted a multicenter, retrospective cohort study, comparing outcomes between intervention and control hospitals within a US eight-hospital urban network. Patients hospitalized with COVID-19 pneumonia between April 13<sup>th</sup>, 2020 and June 19<sup>th</sup>, 2020 were included in the study, which was a time of a regional surge of COVID-19 admissions. An automated, electronic early warning protocol to identify patients with moderate-severe hypoxemia on the medical floors and implement early interventions was implemented at one of the eight hospitals (\"the intervention hospital\").</p><p><strong>Results: </strong>Among 1024 patients, 403 (39%) were admitted to the intervention hospital and 621 (61%) were admitted to one of the control hospitals. Adjusted for potential confounders, patients at the intervention hospital were less likely to be admitted to the ICU (HR = 0.73, 95% CI 0.53, 1.000, <i>P</i> = .0499) compared to the control hospitals. Patients admitted from the floors to the ICU at the intervention hospital had shorter ICU stay (HR for ICU discharge: 1.74; 95% CI 1.21, 2.51, <i>P</i> = .003). There was no significant difference between intervention and control hospitals in need for mechanical ventilation (OR = 0.93; 95% CI 0.38, 2.31; <i>P</i> = .88) or hospital mortality (OR = 0.79; 95% CI 0.52, 1.18; <i>P</i> = .25).</p><p><strong>Conclusion: </strong>A protocol to conserve ICU beds by implementing an early warning system with a dedicated response team to manage respiratory distress on the floors reduced ICU admission and was not associated with worse outcomes compared to hospitals that managed similar levels of respiratory distress in the ICU.</p>","PeriodicalId":44269,"journal":{"name":"Clinical Medicine Insights-Circulatory Respiratory and Pulmonary Medicine","volume":"17 ","pages":"11795484231156755"},"PeriodicalIF":0.9000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/c0/67/10.1177_11795484231156755.PMC10034308.pdf","citationCount":"0","resultStr":"{\"title\":\"Impact of an Early Warning System Protocol, for Patients Admitted to the Medical Floors with SARS-COV2 Pneumonia, on ICU Admission.\",\"authors\":\"Seife Yohannes, Nitin Seam, Junfeng Sun, Joel McAlduff, Janet L Thorne, Susanne B Lara, Michael Keller\",\"doi\":\"10.1177/11795484231156755\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>COVID-19 placed a significant burden on the global healthcare system. Strain in critical care capacity has been associated with increased COVID-19-related ICU mortality. This study evaluates the impact of an early warning system and response team implemented on medical floors to safely triage and care for critically ill patients on the floor and preserve ICU capacity.</p><p><strong>Methods: </strong>We conducted a multicenter, retrospective cohort study, comparing outcomes between intervention and control hospitals within a US eight-hospital urban network. Patients hospitalized with COVID-19 pneumonia between April 13<sup>th</sup>, 2020 and June 19<sup>th</sup>, 2020 were included in the study, which was a time of a regional surge of COVID-19 admissions. An automated, electronic early warning protocol to identify patients with moderate-severe hypoxemia on the medical floors and implement early interventions was implemented at one of the eight hospitals (\\\"the intervention hospital\\\").</p><p><strong>Results: </strong>Among 1024 patients, 403 (39%) were admitted to the intervention hospital and 621 (61%) were admitted to one of the control hospitals. Adjusted for potential confounders, patients at the intervention hospital were less likely to be admitted to the ICU (HR = 0.73, 95% CI 0.53, 1.000, <i>P</i> = .0499) compared to the control hospitals. Patients admitted from the floors to the ICU at the intervention hospital had shorter ICU stay (HR for ICU discharge: 1.74; 95% CI 1.21, 2.51, <i>P</i> = .003). There was no significant difference between intervention and control hospitals in need for mechanical ventilation (OR = 0.93; 95% CI 0.38, 2.31; <i>P</i> = .88) or hospital mortality (OR = 0.79; 95% CI 0.52, 1.18; <i>P</i> = .25).</p><p><strong>Conclusion: </strong>A protocol to conserve ICU beds by implementing an early warning system with a dedicated response team to manage respiratory distress on the floors reduced ICU admission and was not associated with worse outcomes compared to hospitals that managed similar levels of respiratory distress in the ICU.</p>\",\"PeriodicalId\":44269,\"journal\":{\"name\":\"Clinical Medicine Insights-Circulatory Respiratory and Pulmonary Medicine\",\"volume\":\"17 \",\"pages\":\"11795484231156755\"},\"PeriodicalIF\":0.9000,\"publicationDate\":\"2023-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/c0/67/10.1177_11795484231156755.PMC10034308.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical Medicine Insights-Circulatory Respiratory and Pulmonary Medicine\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1177/11795484231156755\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q4\",\"JCRName\":\"RESPIRATORY SYSTEM\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Medicine Insights-Circulatory Respiratory and Pulmonary Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/11795484231156755","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
引用次数: 0
摘要
背景:2019冠状病毒病给全球卫生保健系统带来了沉重负担。重症监护能力的紧张与covid -19相关的ICU死亡率增加有关。本研究评估了在医疗楼层实施的早期预警系统和反应小组的影响,以安全地分诊和护理楼层的危重病人并保持ICU的能力。方法:我们进行了一项多中心、回顾性队列研究,比较了美国八家城市医院网络中干预医院和对照医院的结果。2020年4月13日至2020年6月19日期间因COVID-19肺炎住院的患者被纳入研究,这是该地区COVID-19入院人数激增的时期。在八家医院中的一家("干预医院")实施了自动电子预警方案,以识别医疗楼层的中重度低氧血症患者并实施早期干预措施。结果:1024例患者中,有403例(39%)入住干预医院,621例(61%)入住对照医院。调整潜在混杂因素后,与对照医院相比,干预医院的患者入住ICU的可能性更低(HR = 0.73, 95% CI 0.53, 1.000, P = 0.0499)。干预医院从楼层入住ICU的患者ICU住院时间较短(ICU出院HR: 1.74;95% ci 1.21, 2.51, p = 0.003)。干预医院与对照组需要机械通气的医院间差异无统计学意义(OR = 0.93;95% ci 0.38, 2.31;P = 0.88)或住院死亡率(or = 0.79;95% ci 0.52, 1.18;p = .25)。结论:与管理相似呼吸窘迫水平的医院相比,通过实施早期预警系统和专门的反应小组来管理楼层呼吸窘迫的方案来节省ICU床位,减少了ICU入院率,并且与更差的结果无关。
Impact of an Early Warning System Protocol, for Patients Admitted to the Medical Floors with SARS-COV2 Pneumonia, on ICU Admission.
Background: COVID-19 placed a significant burden on the global healthcare system. Strain in critical care capacity has been associated with increased COVID-19-related ICU mortality. This study evaluates the impact of an early warning system and response team implemented on medical floors to safely triage and care for critically ill patients on the floor and preserve ICU capacity.
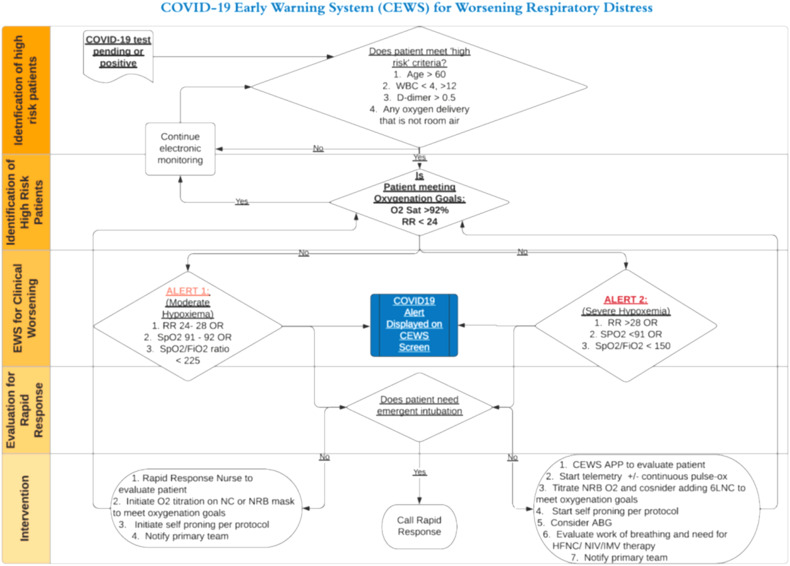
Methods: We conducted a multicenter, retrospective cohort study, comparing outcomes between intervention and control hospitals within a US eight-hospital urban network. Patients hospitalized with COVID-19 pneumonia between April 13th, 2020 and June 19th, 2020 were included in the study, which was a time of a regional surge of COVID-19 admissions. An automated, electronic early warning protocol to identify patients with moderate-severe hypoxemia on the medical floors and implement early interventions was implemented at one of the eight hospitals ("the intervention hospital").
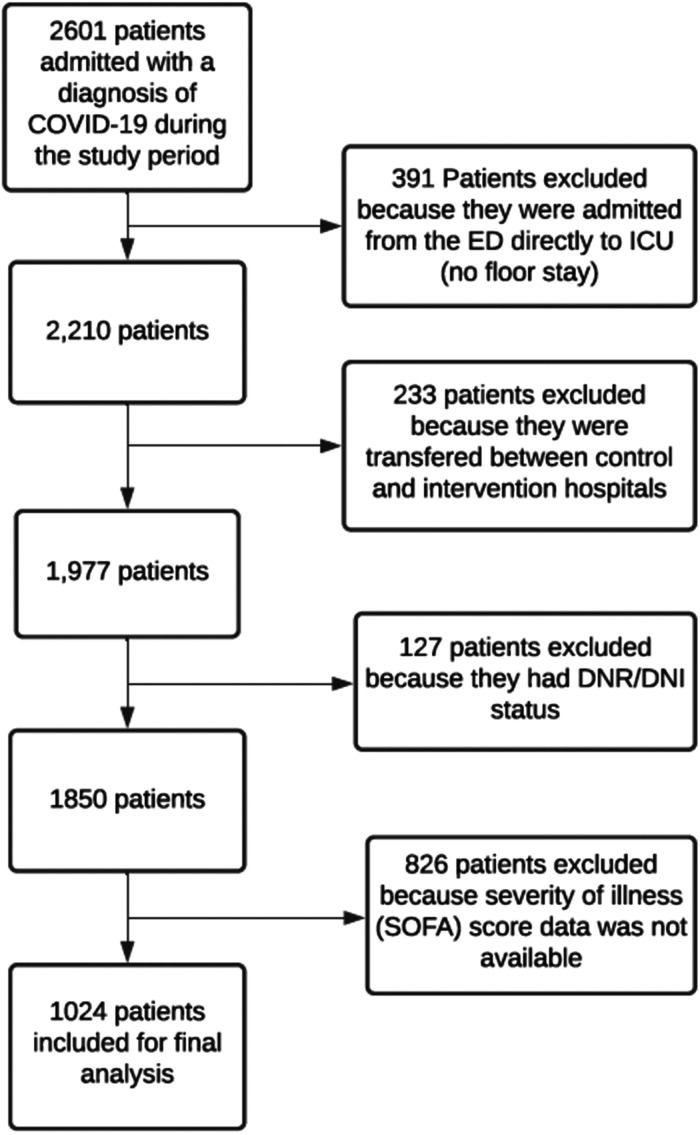
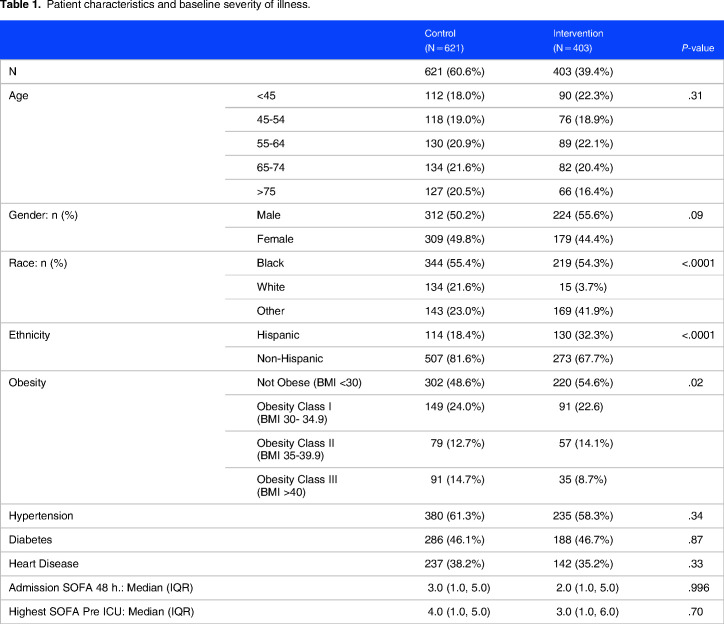
Results: Among 1024 patients, 403 (39%) were admitted to the intervention hospital and 621 (61%) were admitted to one of the control hospitals. Adjusted for potential confounders, patients at the intervention hospital were less likely to be admitted to the ICU (HR = 0.73, 95% CI 0.53, 1.000, P = .0499) compared to the control hospitals. Patients admitted from the floors to the ICU at the intervention hospital had shorter ICU stay (HR for ICU discharge: 1.74; 95% CI 1.21, 2.51, P = .003). There was no significant difference between intervention and control hospitals in need for mechanical ventilation (OR = 0.93; 95% CI 0.38, 2.31; P = .88) or hospital mortality (OR = 0.79; 95% CI 0.52, 1.18; P = .25).
Conclusion: A protocol to conserve ICU beds by implementing an early warning system with a dedicated response team to manage respiratory distress on the floors reduced ICU admission and was not associated with worse outcomes compared to hospitals that managed similar levels of respiratory distress in the ICU.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
