{"title":"对南非四个省的单一直升机紧急医疗服务运营商进行为期12个月的回顾性描述性分析","authors":"Neville Vlok, Craig Wylie, Willem Stassen","doi":"10.1016/j.afjem.2023.05.007","DOIUrl":null,"url":null,"abstract":"<div><h3>Introduction</h3><p>Helicopter Emergency Medical Services (HEMS) is integrated into modern emergency medical services because of its suggested mortality benefit in certain patient populations, it is an expensive resource and appropriate use/feasibility in low- to middle income countries (LMIC) is highly debated. To maximise benefit, correct patient selection in HEMS is paramount. To achieve this, current practices first need to be described. The study aims to describe a population of patients utilising HEMS in South Africa, in terms of flight data, patient demographics, provisional diagnosis, as well as clinical characteristics and interventions.</p></div><div><h3>Methods</h3><p>A retrospective flight- and patient-chart review were conducted, extracting clinical and mission data of a single aeromedical operator in South Africa, over a 12-month period (July 2017 – June 2018) in Gauteng, Free State, Mpumalanga and North-West provinces.</p></div><div><h3>Results</h3><p>A total of 916 cases were included (203 primary cases, 713 interfacility transport (IFT) cases). Most patients transported were male (n=548, 59.8%) and suffered blunt trauma (n=379, 41.4%). Medical pathology (n=247, 27%) and neonatal transfers (n=184, 20.1%) follows. Flights occurred mainly in daylight hours (n=729, 79.6%) with median mission times of 1-hour 53 minutes (primary missions), and 3 hours 10 minutes (IFT missions). Median on-scene times were 26 minutes (primary missions) and 55 minutes (IFT missions). Almost half were transported with an endotracheal tube (n=428, 46.7%), with a large number receiving no respiratory support (n=414, 45.2%). No patients received fibrinolysis, defibrillation, cardioversion or cardiac pacing. Intravenous fluid therapy (n=867, 94.7%) was almost universal, with common administration of sedation (n=430, 46.9%) and analgesia (n=329, 35.9%).</p></div><div><h3>Conclusion</h3><p>Apart from the lack of universal call-out criteria and response to the high burden of trauma, HEMS seem to fulfil an important critical care transport role. It seems that cardiac pathologies are under-represented in this study and might have an important implication for crew training requirements.</p></div>","PeriodicalId":48515,"journal":{"name":"African Journal of Emergency Medicine","volume":"13 3","pages":"Pages 127-134"},"PeriodicalIF":1.3000,"publicationDate":"2023-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10238258/pdf/","citationCount":"1","resultStr":"{\"title\":\"A 12-month retrospective descriptive analysis of a single helicopter emergency medical service operator in four South African provinces\",\"authors\":\"Neville Vlok, Craig Wylie, Willem Stassen\",\"doi\":\"10.1016/j.afjem.2023.05.007\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div><h3>Introduction</h3><p>Helicopter Emergency Medical Services (HEMS) is integrated into modern emergency medical services because of its suggested mortality benefit in certain patient populations, it is an expensive resource and appropriate use/feasibility in low- to middle income countries (LMIC) is highly debated. To maximise benefit, correct patient selection in HEMS is paramount. To achieve this, current practices first need to be described. The study aims to describe a population of patients utilising HEMS in South Africa, in terms of flight data, patient demographics, provisional diagnosis, as well as clinical characteristics and interventions.</p></div><div><h3>Methods</h3><p>A retrospective flight- and patient-chart review were conducted, extracting clinical and mission data of a single aeromedical operator in South Africa, over a 12-month period (July 2017 – June 2018) in Gauteng, Free State, Mpumalanga and North-West provinces.</p></div><div><h3>Results</h3><p>A total of 916 cases were included (203 primary cases, 713 interfacility transport (IFT) cases). Most patients transported were male (n=548, 59.8%) and suffered blunt trauma (n=379, 41.4%). Medical pathology (n=247, 27%) and neonatal transfers (n=184, 20.1%) follows. Flights occurred mainly in daylight hours (n=729, 79.6%) with median mission times of 1-hour 53 minutes (primary missions), and 3 hours 10 minutes (IFT missions). Median on-scene times were 26 minutes (primary missions) and 55 minutes (IFT missions). Almost half were transported with an endotracheal tube (n=428, 46.7%), with a large number receiving no respiratory support (n=414, 45.2%). No patients received fibrinolysis, defibrillation, cardioversion or cardiac pacing. Intravenous fluid therapy (n=867, 94.7%) was almost universal, with common administration of sedation (n=430, 46.9%) and analgesia (n=329, 35.9%).</p></div><div><h3>Conclusion</h3><p>Apart from the lack of universal call-out criteria and response to the high burden of trauma, HEMS seem to fulfil an important critical care transport role. It seems that cardiac pathologies are under-represented in this study and might have an important implication for crew training requirements.</p></div>\",\"PeriodicalId\":48515,\"journal\":{\"name\":\"African Journal of Emergency Medicine\",\"volume\":\"13 3\",\"pages\":\"Pages 127-134\"},\"PeriodicalIF\":1.3000,\"publicationDate\":\"2023-09-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10238258/pdf/\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"African Journal of Emergency Medicine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://www.sciencedirect.com/science/article/pii/S2211419X23000265\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/6/1 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"EMERGENCY MEDICINE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"African Journal of Emergency Medicine","FirstCategoryId":"3","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2211419X23000265","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/6/1 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"EMERGENCY MEDICINE","Score":null,"Total":0}
A 12-month retrospective descriptive analysis of a single helicopter emergency medical service operator in four South African provinces
Introduction
Helicopter Emergency Medical Services (HEMS) is integrated into modern emergency medical services because of its suggested mortality benefit in certain patient populations, it is an expensive resource and appropriate use/feasibility in low- to middle income countries (LMIC) is highly debated. To maximise benefit, correct patient selection in HEMS is paramount. To achieve this, current practices first need to be described. The study aims to describe a population of patients utilising HEMS in South Africa, in terms of flight data, patient demographics, provisional diagnosis, as well as clinical characteristics and interventions.
Methods
A retrospective flight- and patient-chart review were conducted, extracting clinical and mission data of a single aeromedical operator in South Africa, over a 12-month period (July 2017 – June 2018) in Gauteng, Free State, Mpumalanga and North-West provinces.
Results
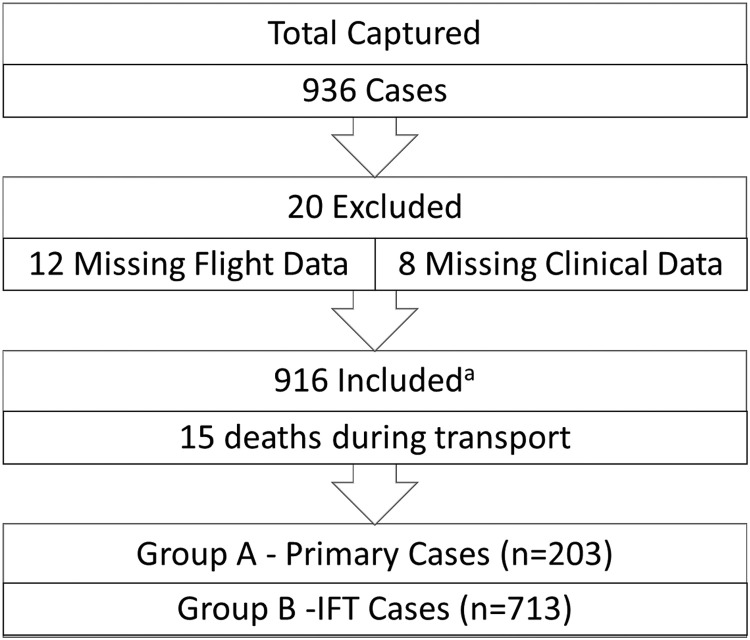
A total of 916 cases were included (203 primary cases, 713 interfacility transport (IFT) cases). Most patients transported were male (n=548, 59.8%) and suffered blunt trauma (n=379, 41.4%). Medical pathology (n=247, 27%) and neonatal transfers (n=184, 20.1%) follows. Flights occurred mainly in daylight hours (n=729, 79.6%) with median mission times of 1-hour 53 minutes (primary missions), and 3 hours 10 minutes (IFT missions). Median on-scene times were 26 minutes (primary missions) and 55 minutes (IFT missions). Almost half were transported with an endotracheal tube (n=428, 46.7%), with a large number receiving no respiratory support (n=414, 45.2%). No patients received fibrinolysis, defibrillation, cardioversion or cardiac pacing. Intravenous fluid therapy (n=867, 94.7%) was almost universal, with common administration of sedation (n=430, 46.9%) and analgesia (n=329, 35.9%).
Conclusion
Apart from the lack of universal call-out criteria and response to the high burden of trauma, HEMS seem to fulfil an important critical care transport role. It seems that cardiac pathologies are under-represented in this study and might have an important implication for crew training requirements.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
