Kelly J Gaffney, Theresa A Urban, Mariana Lucena, Lisa Rybicki, Navneet S Majhail, Sherif Beniameen Mossad
{"title":"异基因造血干细胞移植前预防使用甲氧苄啶-磺胺甲恶唑。","authors":"Kelly J Gaffney, Theresa A Urban, Mariana Lucena, Lisa Rybicki, Navneet S Majhail, Sherif Beniameen Mossad","doi":"10.1007/s44228-023-00029-7","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Our institution has used trimethoprim-sulfamethoxazole (TMP-SMX) as the antibacterial agent of choice for infection prophylaxis during the pre-engraftment period in the allogeneic transplant (allo-HCT) population.</p><p><strong>Methods: </strong>This retrospective, single center study was developed to compare the safety of that antibacterial prophylaxis to fluoroquinolones in allo-HCT. The primary endpoint was time to neutrophil engraftment.</p><p><strong>Results: </strong>A total of 366 patients were reviewed (TMP-SMX n = 332, fluoroquinolone n = 34). No difference in days to neutrophil engraftment was found (median 15 versus 16 days, p = 0.62). Hyperkalemia was more common in the TMP-SMX cohort (32.2% versus 14.7%, p = 0.035); this did not contribute to a higher rate of agent discontinuation or arrhythmia. There was no significant difference in the incidence of neutropenic fever; however, those in the TMP-SMX cohort were more likely to have microbiologically confirmed bacteremia (24.1% versus 8.8% respectively, p = 0.043). There was no significant difference in infections. No long-term implication of prophylactic antibacterial agent selection was observed in terms of graft-versus-host-disease, underlying disease relapse, or mortality.</p><p><strong>Conclusion: </strong>The use of TMP-SMX was associated with a higher likelihood of bacteremia and hyperkalemia; however, this did not result in increased hospital stay, escalation of care, or mortality. The use of TMP-SMX for prophylaxis during the pre-engraftment period for allo-HCT recipients is safe and effective.</p>","PeriodicalId":10368,"journal":{"name":"Clinical Hematology International","volume":"5 2-3","pages":"65-70"},"PeriodicalIF":0.0000,"publicationDate":"2023-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10241755/pdf/","citationCount":"2","resultStr":"{\"title\":\"Prophylactic Trimethoprim-Sulfamethoxazole for Allogeneic Hematopoietic Stem Cell Transplant Recipients During the Pre-engraftment Period.\",\"authors\":\"Kelly J Gaffney, Theresa A Urban, Mariana Lucena, Lisa Rybicki, Navneet S Majhail, Sherif Beniameen Mossad\",\"doi\":\"10.1007/s44228-023-00029-7\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Our institution has used trimethoprim-sulfamethoxazole (TMP-SMX) as the antibacterial agent of choice for infection prophylaxis during the pre-engraftment period in the allogeneic transplant (allo-HCT) population.</p><p><strong>Methods: </strong>This retrospective, single center study was developed to compare the safety of that antibacterial prophylaxis to fluoroquinolones in allo-HCT. The primary endpoint was time to neutrophil engraftment.</p><p><strong>Results: </strong>A total of 366 patients were reviewed (TMP-SMX n = 332, fluoroquinolone n = 34). No difference in days to neutrophil engraftment was found (median 15 versus 16 days, p = 0.62). Hyperkalemia was more common in the TMP-SMX cohort (32.2% versus 14.7%, p = 0.035); this did not contribute to a higher rate of agent discontinuation or arrhythmia. There was no significant difference in the incidence of neutropenic fever; however, those in the TMP-SMX cohort were more likely to have microbiologically confirmed bacteremia (24.1% versus 8.8% respectively, p = 0.043). There was no significant difference in infections. No long-term implication of prophylactic antibacterial agent selection was observed in terms of graft-versus-host-disease, underlying disease relapse, or mortality.</p><p><strong>Conclusion: </strong>The use of TMP-SMX was associated with a higher likelihood of bacteremia and hyperkalemia; however, this did not result in increased hospital stay, escalation of care, or mortality. The use of TMP-SMX for prophylaxis during the pre-engraftment period for allo-HCT recipients is safe and effective.</p>\",\"PeriodicalId\":10368,\"journal\":{\"name\":\"Clinical Hematology International\",\"volume\":\"5 2-3\",\"pages\":\"65-70\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-06-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10241755/pdf/\",\"citationCount\":\"2\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical Hematology International\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1007/s44228-023-00029-7\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Hematology International","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1007/s44228-023-00029-7","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Prophylactic Trimethoprim-Sulfamethoxazole for Allogeneic Hematopoietic Stem Cell Transplant Recipients During the Pre-engraftment Period.
Background: Our institution has used trimethoprim-sulfamethoxazole (TMP-SMX) as the antibacterial agent of choice for infection prophylaxis during the pre-engraftment period in the allogeneic transplant (allo-HCT) population.
Methods: This retrospective, single center study was developed to compare the safety of that antibacterial prophylaxis to fluoroquinolones in allo-HCT. The primary endpoint was time to neutrophil engraftment.
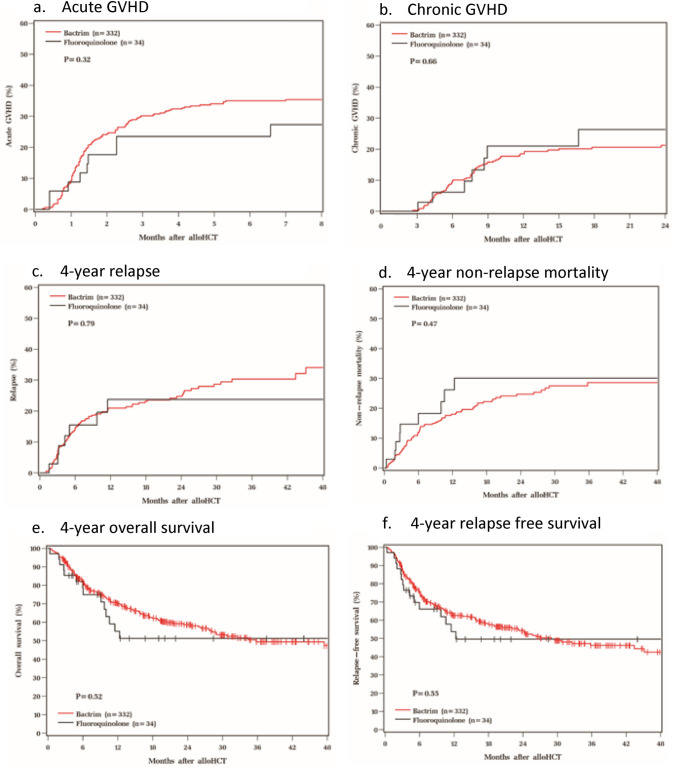
Results: A total of 366 patients were reviewed (TMP-SMX n = 332, fluoroquinolone n = 34). No difference in days to neutrophil engraftment was found (median 15 versus 16 days, p = 0.62). Hyperkalemia was more common in the TMP-SMX cohort (32.2% versus 14.7%, p = 0.035); this did not contribute to a higher rate of agent discontinuation or arrhythmia. There was no significant difference in the incidence of neutropenic fever; however, those in the TMP-SMX cohort were more likely to have microbiologically confirmed bacteremia (24.1% versus 8.8% respectively, p = 0.043). There was no significant difference in infections. No long-term implication of prophylactic antibacterial agent selection was observed in terms of graft-versus-host-disease, underlying disease relapse, or mortality.
Conclusion: The use of TMP-SMX was associated with a higher likelihood of bacteremia and hyperkalemia; however, this did not result in increased hospital stay, escalation of care, or mortality. The use of TMP-SMX for prophylaxis during the pre-engraftment period for allo-HCT recipients is safe and effective.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
