Sara Bowman, Joe Stanek, Rajinder Bajwa, Veronika Polishchuk, Rolla Abu-Arja, Hemalatha G Rangarajan
{"title":"儿童同种异体干细胞移植受者的CD34干细胞增加:病例系列和文献综述。","authors":"Sara Bowman, Joe Stanek, Rajinder Bajwa, Veronika Polishchuk, Rolla Abu-Arja, Hemalatha G Rangarajan","doi":"10.1007/s44228-023-00042-w","DOIUrl":null,"url":null,"abstract":"<p><p>Patients with poor graft function (PGF) or declining donor chimerism (DC) post allogeneic hematopoietic cell transplantation (HCT) may benefit from a CD34-selected stem cell boost (SCB). We retrospectively studied outcomes of fourteen pediatric patients (PGF: 12 and declining DC: 2), with a median age of 12.8 (range 0.08-20.6) years at HCT, who received a SCB. Primary and secondary endpoints included resolution of PGF or improvement in DC (≥ 15% increase), overall survival (OS) and transplant-related mortality (TRM), respectively. The median CD34 dose infused was 7.47 × 10<sup>6</sup>/kg (range 3.51 × 10<sup>6</sup>-3.39 × 10<sup>7</sup>/kg). Among patients with PGF who survived ≥ 3 months post-SCB (n = 8), we observed a non-significant decrease in the cumulative median number of red cell transfusions, platelet transfusions, and GCSF but not intravenous immunoglobulin doses in the 3 months before and after SCB. Overall response rate (ORR) was 50%, with 29% complete and 21% partial responses. ORR was better in recipients who received lymphodepletion (LD) pre-SCB versus none (75% versus 40%; p = 0.56). The incidence of acute and chronic graft-versus-host-disease was 7% and 14%, respectively. The 1-year OS was 50% (95% CI 23-72%) and TRM was 29% (95% CI 8-58%). SCB was effective in half of our cohort with possible benefit of LD pre-SCB.</p>","PeriodicalId":10368,"journal":{"name":"Clinical Hematology International","volume":"5 2-3","pages":"155-164"},"PeriodicalIF":0.0000,"publicationDate":"2023-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10241744/pdf/","citationCount":"0","resultStr":"{\"title\":\"CD34 Stem Cell Boost in Pediatric Allogeneic Stem Cell Transplant Recipients: A Case Series and Review of Literature.\",\"authors\":\"Sara Bowman, Joe Stanek, Rajinder Bajwa, Veronika Polishchuk, Rolla Abu-Arja, Hemalatha G Rangarajan\",\"doi\":\"10.1007/s44228-023-00042-w\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Patients with poor graft function (PGF) or declining donor chimerism (DC) post allogeneic hematopoietic cell transplantation (HCT) may benefit from a CD34-selected stem cell boost (SCB). We retrospectively studied outcomes of fourteen pediatric patients (PGF: 12 and declining DC: 2), with a median age of 12.8 (range 0.08-20.6) years at HCT, who received a SCB. Primary and secondary endpoints included resolution of PGF or improvement in DC (≥ 15% increase), overall survival (OS) and transplant-related mortality (TRM), respectively. The median CD34 dose infused was 7.47 × 10<sup>6</sup>/kg (range 3.51 × 10<sup>6</sup>-3.39 × 10<sup>7</sup>/kg). Among patients with PGF who survived ≥ 3 months post-SCB (n = 8), we observed a non-significant decrease in the cumulative median number of red cell transfusions, platelet transfusions, and GCSF but not intravenous immunoglobulin doses in the 3 months before and after SCB. Overall response rate (ORR) was 50%, with 29% complete and 21% partial responses. ORR was better in recipients who received lymphodepletion (LD) pre-SCB versus none (75% versus 40%; p = 0.56). The incidence of acute and chronic graft-versus-host-disease was 7% and 14%, respectively. The 1-year OS was 50% (95% CI 23-72%) and TRM was 29% (95% CI 8-58%). SCB was effective in half of our cohort with possible benefit of LD pre-SCB.</p>\",\"PeriodicalId\":10368,\"journal\":{\"name\":\"Clinical Hematology International\",\"volume\":\"5 2-3\",\"pages\":\"155-164\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-06-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10241744/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical Hematology International\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1007/s44228-023-00042-w\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Hematology International","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1007/s44228-023-00042-w","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
摘要
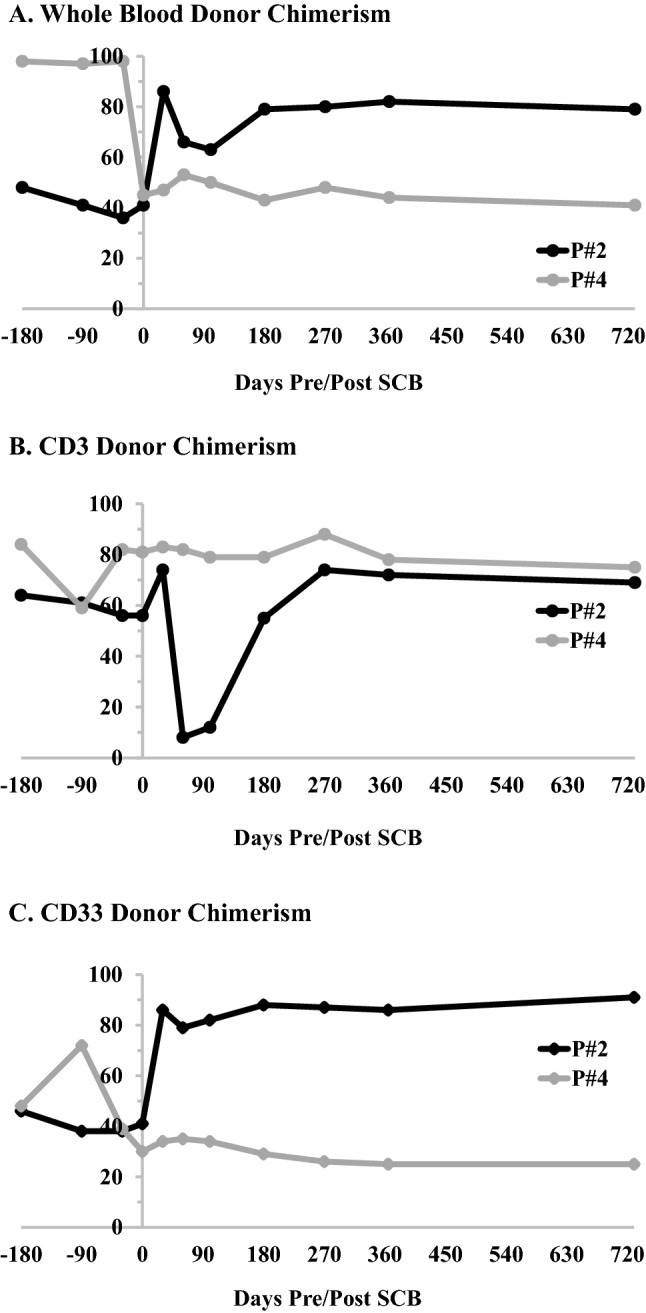
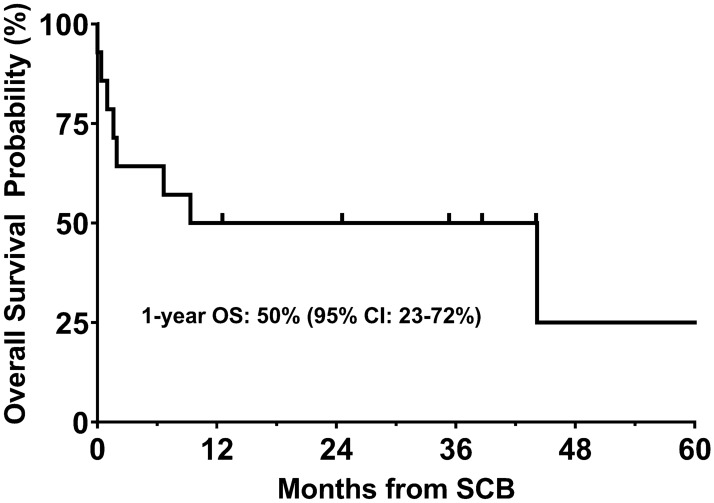
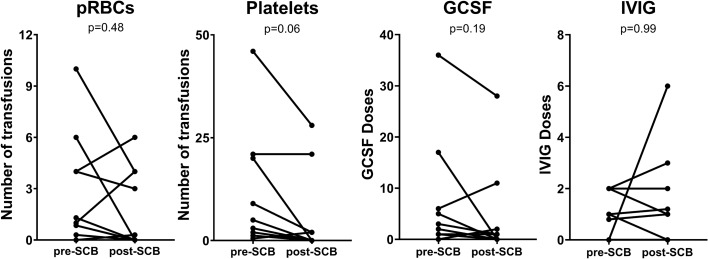
同种异体造血细胞移植(HCT)后移植物功能差(PGF)或供体嵌合(DC)下降的患者可能受益于cd34选择的干细胞增强(SCB)。我们回顾性研究了14例接受SCB的儿童患者(PGF: 12, DC: 2下降),HCT的中位年龄为12.8岁(范围0.08-20.6)。主要终点和次要终点分别包括PGF的消退或DC的改善(增加≥15%)、总生存期(OS)和移植相关死亡率(TRM)。注射CD34的中位剂量为7.47 × 106/kg (3.51 × 106 ~ 3.39 × 107/kg)。在SCB后存活≥3个月的PGF患者中(n = 8),我们观察到红细胞输注、血小板输注和GCSF的累积中位数在SCB前后3个月内无显著下降,但静脉注射免疫球蛋白剂量无显著下降。总缓解率(ORR)为50%,其中29%为完全缓解,21%为部分缓解。接受淋巴细胞清除(LD)前scb治疗的患者ORR优于未接受治疗的患者(75% vs 40%;p = 0.56)。急性和慢性移植物抗宿主病的发生率分别为7%和14%。1年OS为50% (95% CI 23-72%), TRM为29% (95% CI 8-58%)。SCB在我们的队列中有一半有效,可能受益于LD前SCB。
CD34 Stem Cell Boost in Pediatric Allogeneic Stem Cell Transplant Recipients: A Case Series and Review of Literature.
Patients with poor graft function (PGF) or declining donor chimerism (DC) post allogeneic hematopoietic cell transplantation (HCT) may benefit from a CD34-selected stem cell boost (SCB). We retrospectively studied outcomes of fourteen pediatric patients (PGF: 12 and declining DC: 2), with a median age of 12.8 (range 0.08-20.6) years at HCT, who received a SCB. Primary and secondary endpoints included resolution of PGF or improvement in DC (≥ 15% increase), overall survival (OS) and transplant-related mortality (TRM), respectively. The median CD34 dose infused was 7.47 × 106/kg (range 3.51 × 106-3.39 × 107/kg). Among patients with PGF who survived ≥ 3 months post-SCB (n = 8), we observed a non-significant decrease in the cumulative median number of red cell transfusions, platelet transfusions, and GCSF but not intravenous immunoglobulin doses in the 3 months before and after SCB. Overall response rate (ORR) was 50%, with 29% complete and 21% partial responses. ORR was better in recipients who received lymphodepletion (LD) pre-SCB versus none (75% versus 40%; p = 0.56). The incidence of acute and chronic graft-versus-host-disease was 7% and 14%, respectively. The 1-year OS was 50% (95% CI 23-72%) and TRM was 29% (95% CI 8-58%). SCB was effective in half of our cohort with possible benefit of LD pre-SCB.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
