Oscar Selvaggio, Ugo Giovanni Falagario, Marco Finati, Salvatore Mariano Bruno, Marco Recchia, Paola Milillo, Francesca Sanguedolce, Giovanni Silecchia, Luca Macarini, Luigi Cormio, Giuseppe Carrieri
{"title":"全陆地冷冻消融治疗前列腺癌症和高淋巴结侵袭风险患者的肿瘤结果。","authors":"Oscar Selvaggio, Ugo Giovanni Falagario, Marco Finati, Salvatore Mariano Bruno, Marco Recchia, Paola Milillo, Francesca Sanguedolce, Giovanni Silecchia, Luca Macarini, Luigi Cormio, Giuseppe Carrieri","doi":"10.4103/ua.ua_171_21","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>Prostate cryoablation has been proposed as an alternative to radical prostatectomy for men with localized prostate cancer (PCa); however, it is limited by the lack of data regarding oncological outcomes and the impossibility of performing a lymph node dissection. The aim of this study was to assess if whole-gland cryoablation is oncologically safe, especially for patients in whom pelvic lymph node dissection would be necessary.</p><p><strong>Materials and methods: </strong>After institutional review board approval, we identified 102 patients who underwent whole-gland prostate cryoablation between 2013 and April 2019. Lymph node invasion (LNI) probability was computed using Briganti nomogram, and a 5% cutoff probability was used to stratify the population in two groups. Biochemical recurrence after procedure was assessed using Phoenix criteria. Multiparametric magnetic resonance imaging, (CT), and bone scan or choline positron-emission tomography/CT were performed for the detection of distant metastases.</p><p><strong>Results: </strong>Seventeen (17%) patients were treated for a low-risk PCa, 48 (47%) patients were at intermediate-risk PCa, and 37 (36%) patients were at high-risk PCa. Patients with a probability of LNI >5% (<i>n</i> = 46) exhibited higher prostate-specific antigen (PSA), PSA density, ISUP Grade Group, CT stage, and european association of urology (EAU) risk. Recurrence-free survival rates at 3 years' follow-up were 93%, 82%, and 72%, respectively for low-, intermediate-, and high-risk patients. At a median follow-up of 37 months (17-62), additional treatment and metastasis-free survival were 84% and 97%, respectively. No differences in oncological outcomes were found in patients with a probability of LNI above and below 5%.</p><p><strong>Conclusions: </strong>Prostate whole-gland cryoablation can be considered a safe procedure with acceptable outcomes in low- and intermediate-risk patients. A high preoperative risk of nodal involvement could not be considered an exclusion criterion to perform cryoablation. Further studies are required.</p>","PeriodicalId":23633,"journal":{"name":"Urology Annals","volume":"15 1","pages":"48-53"},"PeriodicalIF":0.8000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/80/93/UA-15-48.PMC10062521.pdf","citationCount":"0","resultStr":"{\"title\":\"Oncological outcomes of whole-gland cryoablation in patients with prostate cancer and high risk of lymph node invasion.\",\"authors\":\"Oscar Selvaggio, Ugo Giovanni Falagario, Marco Finati, Salvatore Mariano Bruno, Marco Recchia, Paola Milillo, Francesca Sanguedolce, Giovanni Silecchia, Luca Macarini, Luigi Cormio, Giuseppe Carrieri\",\"doi\":\"10.4103/ua.ua_171_21\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Purpose: </strong>Prostate cryoablation has been proposed as an alternative to radical prostatectomy for men with localized prostate cancer (PCa); however, it is limited by the lack of data regarding oncological outcomes and the impossibility of performing a lymph node dissection. The aim of this study was to assess if whole-gland cryoablation is oncologically safe, especially for patients in whom pelvic lymph node dissection would be necessary.</p><p><strong>Materials and methods: </strong>After institutional review board approval, we identified 102 patients who underwent whole-gland prostate cryoablation between 2013 and April 2019. Lymph node invasion (LNI) probability was computed using Briganti nomogram, and a 5% cutoff probability was used to stratify the population in two groups. Biochemical recurrence after procedure was assessed using Phoenix criteria. Multiparametric magnetic resonance imaging, (CT), and bone scan or choline positron-emission tomography/CT were performed for the detection of distant metastases.</p><p><strong>Results: </strong>Seventeen (17%) patients were treated for a low-risk PCa, 48 (47%) patients were at intermediate-risk PCa, and 37 (36%) patients were at high-risk PCa. Patients with a probability of LNI >5% (<i>n</i> = 46) exhibited higher prostate-specific antigen (PSA), PSA density, ISUP Grade Group, CT stage, and european association of urology (EAU) risk. Recurrence-free survival rates at 3 years' follow-up were 93%, 82%, and 72%, respectively for low-, intermediate-, and high-risk patients. At a median follow-up of 37 months (17-62), additional treatment and metastasis-free survival were 84% and 97%, respectively. No differences in oncological outcomes were found in patients with a probability of LNI above and below 5%.</p><p><strong>Conclusions: </strong>Prostate whole-gland cryoablation can be considered a safe procedure with acceptable outcomes in low- and intermediate-risk patients. A high preoperative risk of nodal involvement could not be considered an exclusion criterion to perform cryoablation. Further studies are required.</p>\",\"PeriodicalId\":23633,\"journal\":{\"name\":\"Urology Annals\",\"volume\":\"15 1\",\"pages\":\"48-53\"},\"PeriodicalIF\":0.8000,\"publicationDate\":\"2023-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/80/93/UA-15-48.PMC10062521.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Urology Annals\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.4103/ua.ua_171_21\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2022/11/8 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q4\",\"JCRName\":\"UROLOGY & NEPHROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Urology Annals","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4103/ua.ua_171_21","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/11/8 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
Oncological outcomes of whole-gland cryoablation in patients with prostate cancer and high risk of lymph node invasion.
Purpose: Prostate cryoablation has been proposed as an alternative to radical prostatectomy for men with localized prostate cancer (PCa); however, it is limited by the lack of data regarding oncological outcomes and the impossibility of performing a lymph node dissection. The aim of this study was to assess if whole-gland cryoablation is oncologically safe, especially for patients in whom pelvic lymph node dissection would be necessary.
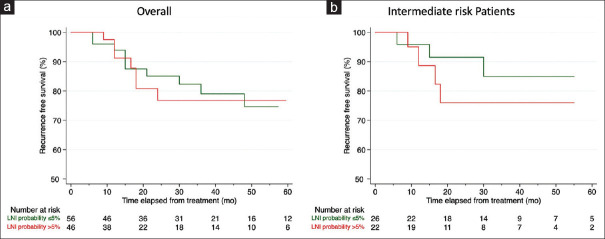
Materials and methods: After institutional review board approval, we identified 102 patients who underwent whole-gland prostate cryoablation between 2013 and April 2019. Lymph node invasion (LNI) probability was computed using Briganti nomogram, and a 5% cutoff probability was used to stratify the population in two groups. Biochemical recurrence after procedure was assessed using Phoenix criteria. Multiparametric magnetic resonance imaging, (CT), and bone scan or choline positron-emission tomography/CT were performed for the detection of distant metastases.
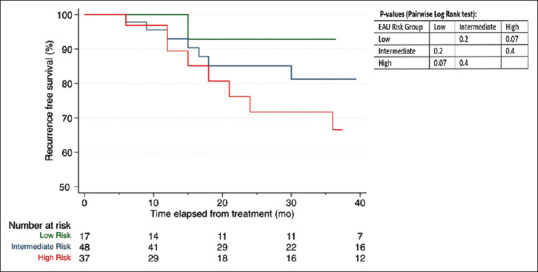
Results: Seventeen (17%) patients were treated for a low-risk PCa, 48 (47%) patients were at intermediate-risk PCa, and 37 (36%) patients were at high-risk PCa. Patients with a probability of LNI >5% (n = 46) exhibited higher prostate-specific antigen (PSA), PSA density, ISUP Grade Group, CT stage, and european association of urology (EAU) risk. Recurrence-free survival rates at 3 years' follow-up were 93%, 82%, and 72%, respectively for low-, intermediate-, and high-risk patients. At a median follow-up of 37 months (17-62), additional treatment and metastasis-free survival were 84% and 97%, respectively. No differences in oncological outcomes were found in patients with a probability of LNI above and below 5%.
Conclusions: Prostate whole-gland cryoablation can be considered a safe procedure with acceptable outcomes in low- and intermediate-risk patients. A high preoperative risk of nodal involvement could not be considered an exclusion criterion to perform cryoablation. Further studies are required.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
